
Overview

Problem

Technical Wall

Design Pivot
System Impact

Outcomes



Overview
Problem
Technical Wall
Design Pivot
System Impact

Retrospective
Overview
Designing AI Continuity in High Stakes Systems
Healthcare workflows break not because of a lack of data. They break because context doesn’t survive transitions.
Problem Framing
Stabilize Continuity • Predictive Reasoning • Not Automate Decisions
Why This Matters
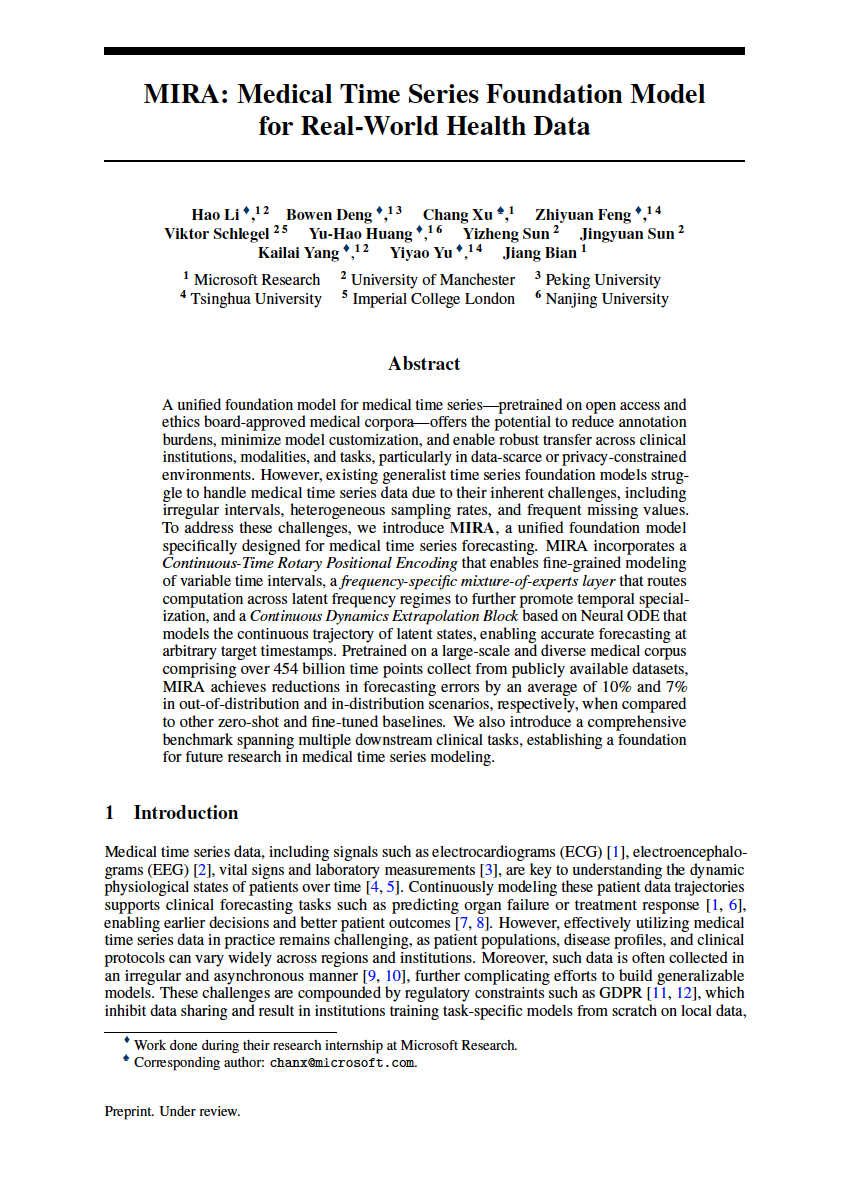
Recent research highlights the importance of understanding patient state over time, not just at isolated moments.
MIRA: A Medical Foundation Model (NeurIPS)
Explores longitudinal modeling of medical data to enable more holistic insights across conditions.
This project applies that insight at the workflow level:
How continuity can be preserved across roles, systems, and handoffs without replacing human judgment.
The Hero Problem
Clinical continuity breaks across role boundaries and system transitions, forcing humans to rebuild context manually
High Cognitive Load • Repeated Work • Trust Gaps in AI tools
5 Day Product Design Sprint – From Discovery to Prototype
From scattered point points to a shared systemic problem
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5

Problem Locked

Concept Selected

Prototype Ready
Objectives
Problem Framing
Analyze Current State
Ideate & Select
Build Prototype
Present & Plan
Research
& Discovery
Analyze current state
Synthesis
Current-State Mapping
Systems
& Design Thinking
Failure Analysis
AI Opportunity Framing
Prototyping
Low-fidelity flows
Core Flow Prototype
Persona Summaries
Final Narrative & Metrics
Deliverables
Workflow Diagram
Low-Fi Screens
Rapid Prototypes
The Problem & Discovery
Mapping the Shared Reality
From Retrieval to Proactive Delivery – The AI Layer
Identifying how Nurses, Physicians, and Specialists interact with data during crisis moments
Discovery & Interviews

Who I Spoke With
- Child & Adolescent Psychiatrist
- OB/GYN
- Maternal Fetal Medicine Physician (MFM)
- Registered Nurse (RN)
- Registration / Admin



What I Listened For
- Handoffs
- Cognitive load
- Risk points
- Trust boundaries
- AI adoption barriers

Physicians
“So many of our decisions are time-sensitive, but the information we need is often incomplete or scattered. I’m constantly double-checking because I don’t trust that I’m seeing the full picture.”
Breaks Today
Fragmented context, repeated documentation, low trust in prior data
Needs
Clear deltas, confidence-scored risks, evidence with human override

Nurses
“I’m interrupted constantly. I rely on quick signals to know what actually matters right now, but I still end up manually checking charts to make sure nothing critical was missed.”
Breaks Today
Interruptions, alert overload, manual safety checks
Needs
Prioritized tasks, trend signals, shift-safe handoffs

Admins
“When information is missing or changes without warning, we’re the ones trying to fix it. A small data issue upstream can turn into scheduling failures and patient frustration.”
Breaks Today
Missing context, silent automation failures, unclear urgency
Needs
Early risk signals, dependency visibility, auditable fixes
Emerging Themes & Cross-role Patterns
This validated continuity as a systemic problem, not UI issues
- Timing-sensitive decisions with incomplete data
- AI tools that help in isolation, but don’t connect the system
- Manual verification loops
- Repeated documentation
- Context loss at handoffs
Emerging Problem Themes Across the Clinical Continuity Ecosystem
Patterns observed across clinicians, operations, and frontline care during discovery interviews

High-risk convergence across roles
Localized role friction
The Technical Wall
From Retrieval to Proactive Context
Why clinicians are forced to rebuild context by hand
Current-State Clinical Workflow: Fragmented Continuity of Care
Where Fragmentation, Repetition, and Trust Gaps Occur
Human Input
Decision Moment
Operational Systems
External Sources
EHR System (CoreHealth)
Info Artifact
View Failure Points
7
Human Touchpoint’s
(Many-to-Many Communication Load)
4
External Data Sources
(Many-to-Many Fragmentation Risk)
4
High-Stakes
Decision Moments
1
Central EHR Record
(Single Source of Truth, Limited Context)
7
Operational Systems per Patient Journey
(1-to-Many Integration Burden)
Fragmented Inputs Create Hidden Clinical Risk
Care teams must coordinate across multiple human handoffs, disconnected operational systems, and incomplete external records. The EHR acts as a central hub, but critical context remains distributed, forcing clinicians to bridge gaps manually during high-stakes decision moments.
AI Opportunity Framework
Two complementary AI Layers Working Together
JSON-AI Layer
(Structured Intelligence)
Structured continuity intelligence
- Medication reconciliation
- Scheduling logic & insurance verification
- Clean summaries
- Continuity “checklist” generation
TOON-AI Layer
(Narrative/Reasoning AI)
Interpretive reasoning
- Nuance-finding in handoffs
- Rick deltas
- Inconsistencies in the patient story
- Reasoning across notes and conversations
- Role-specific briefings
AI restores context so human judgment can be used with confidence
Future-State: AI Continuity Platform Across the Care Journey
A clean, technical systems diagram showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
Design Pivot
Designing the Clinical Intelligence Layer
Different surfaces. Same continuity intelligence
Continuity cannot live in a single interface. It must persist across roles, tools, and time
Three Patterns for AI-Supported Continuity
To avoid “Dashboard Fatigue,” we can move explainability to the object level. Each insight adapts to the persona while utilizing three core patterns.

Continuity Strip
- Explainable, cross-system, non-blocking
- Persistent continuity without competing with system alerts

Sidecar Panel
- System memory across roles and time
- Handoffs, overrides, and reasoning in one place

Shared Timeline
- Moment-of-decision context
- What changed, what matters now, What is next
Persona-Specific Workflows
AI utility is not one-size-fits-all
The system surfaces the same “Intelligence Object” in different formats depending on the user’s role” Physicians receive deep-dive rationale for diagnosis, Nurses see actionable safety threads during handoff, and Admins receive operational status updates to clear discharge bottlenecks.

One Critical Event, Three Interpretations
An external record from St. Mary’s Hospital arrives at 08:42 AM, revealing HIGH-RISK PENICILLIN ALLERGY not documented in the Epic chart. The AI detects this discrepancy and surfaces it differently for each decision owner’s specific pressure points.

Dr. Aris Chen
Attending Physician
Primary Goal
Validate diagnostic risk & maintain accuracy
Decision Pressure Points:
- Deep work mode, cannot tolerate interruptions
- Needs full evidence trail for liability
- Must understand "why" before acting
UI Pattern: The Sidecar Panel
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.

Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream


AI Continuity

Context for this shift
Patient Insights
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Evidence Trail
St. Mary’s discharge summary (02/10) • Confirmed via FHIR import • Verified anaphylaxis history

The Clinical Handshake:

Verify & Update Chart

Flag as Error
Human remains final authority. Action logged to audit trail.

Sarah Martinez, RN
Charge Nurse
Primary Goal
Execute safe tasks during handoff
Decision Pressure Points:
- High task density—needs glanceable safety checks
- Shift handoff = critical error window
- Must act fast without missing context
UI Pattern: The Shared Timeline
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.

Medication Administration


Scheduled Administration
10:00
Amoxicillin 500mg PO


ALLERGY CONFLICT
Critical
Penicillin allergy detected in external record. Amoxicillin is contraindicated.

HIGH
94% Confidence
Auto-flagged

Scheduled assessment
14:00
Amoxicillin 500mg PO
The Clinical Handshake:

Hold Medication
Page Provider
Error prevented. Intervention escalated to physician.

Marcus Kim
Care Coordinator
Primary Goal
Clear discharge bottlenecks & ensure compliance
Decision Pressure Points:
- Manages 40+ patients and needs status at-a-glance
- Doesn’t need clinical PII< just completion status
- Discharge delays = throughput bottlenecks
UI Pattern: Exception-Based Alert Feed
No dashboard to monitor. System PUSHES critical blockers to the feed. Silent when everything flows smoothly.
Active Discharge Blocker Detected

Patient 847-2931
Ready
Patient 847-2931
✓ Now Complete
Status Update
Critical data gap resolved at 08:47

Allergy record reconciled & verified

Patient 847-2931
Pending...
The Clinical Handshake:
Mark Discharge-Ready

View Full Feed
Bottleneck cleared. Patient ready for discharge workflow.
The Clinical Handshake: Closing the Loop
Regardless of role, every interaction ends in a HANDSHAKE. A deliberate human action that confirms or rejects the AI’s synthesis. This ensures that while the AI handles the data plumbing, the human remains the final authority in the clinical record.

Physician
Verify & update with full audit trail

Nurse
Hold medication & escalate to provider

Admin
Mark complete & clear bottleneck
Structural Evolution
From fragmented workspaces to AI-curated chronology
Before
Fragmented Workspaces
TAB CHAOS

Patient

Labs


Med Rec
+8

Verbal Note (Tab 1)
“Patient reports taking Metformin...”
Nurse intake 02/13

Outside PDF (Tab 3)
St. Mary's Hospital Discharge Summary
Scanned: 01/10/2026

Lab Result (Tab 2)
Troponin: 0.8 ng/mL
01/12/2026 13:34

Med Rec (Tab 4)
“Patient reports taking Metformin...”

103 days old



Manual
Integration
After
AI-Curated Timeline
UNIFIED CHRONOLOGY

Shared Timeline
Patient: Sarah Chen
MRN: 847-2934 | Age: 67

Outside Hospital Discharge
02/10/ 14:22
St. Mary’s Hospital • Cardiac Event
JSON-AI auto-parsed PDF

Matched: Discharge RX → Pharmacy

Pharmacy Fill
Metformin 1000mg BID • CVS Pharmacy
TOON-AI linked to discharge orders
02/10/ 16:45
Verified: Nurse note ↔ Pharmacy

Lab Result Anomaly
Troponin I: 0.8 ng/mL ↑ (Critical)
JSON-AI flagged spike pattern
02/12/ 08:34
Linked: Cardiac event → Lab spike
Intake Verification
Nurse confirmed Metformin use verbally
TOON-AI reconciled with CVS record
02/13/ 07:12
Matched: Discharge RX → Parmacy

AI-Insight
Med discrepancy + cardiac markers = High-risk patterns
Now
HIGH
94% Confidence
Auto-flagged before first dose
The Clinical Handshake: Closing the Loop

Problem
Data fragmentation forces clinicians to become “human middleware,” manually integrating disparate sources.

Solution
AI becomes the integration layer, automatically reconciling cross-system data into a unified temporal model.

Impact
Clinicians focus on care decisions, not data archeaology. Critical patterns emerge from temporal synthesis
Action vs. Priority
Preventing Compliance Fatigue
In high-stakes systems, you must distinguish between Actionable Intelligence and Critical Awareness
If you force an "Action" on everything that is "High Priority," you create a "Compliance UI" where users click "OK" just to clear the screen—which is how major medical errors happen.

The Compliance Fatigue Problem
Traditional alert systems conflate Priority (clinical urgency) with Action Required (system needs input). This creates alert fatigue where clinicians dismiss critical warnings just to continue working, leading to preventable medical errors.
Intelligence Action Taxonomy Matrix
Decoupling Action from Urgency
Timeline Visual System
Multimodal Encoding
Progressive disclosure through three-stage scaling and verification state encoding
Icons are hard to see in passive timeline views. This system maintains clarity without cluttering the screen through intelligent scale transitions and semantic color+glyph pairing.
Three-Stage Scaling Strategy
Progressive visual complexity based on user engagement level

16px

Stage 1: Passive
Small dot only. No icon. Keeps the "spine" clean for scrolling through long timelines. Low cognitive load.

32px on hover

Stage 2: Focus
On hover/scroll proximity, node expands to 16px and white glyph fades in. The "Aha!" moment where category is confirmed.
L1: Medication Order
L2: Verified by clinician
02/12 14:08
24px icon in card header

Stage 3: Object
Inside Intel Object Card, icon appears at 24px next to L1 Signal text. Full context revealed.
Why These Patterns
Tradeoffs Under Real-world Constraints
Patterns were selected to fit real systems, not idealized workflows
These patterns were chosen to:
- Respect existing systems of record
- Work across multiple environments
- Minimize workflow disruption
- Allow trust to build incrementally
Why not dashboards?
They centralize information but pull users out of real workflows.
Why not alerts everywhere?
They compete with native warnings and accelerate alert fatigue.
Why not overlays by default?
They interrupt primary tasks and don’t scale across systems.
Structural Evolution
From fragmented workspaces to AI-curated chronology
Anatomy of a Clinical Intelligence Object
A four-layer metadata hierarchy ensuring explainability through Signal,Insight, Rationale, and Evidence
L1
Insight
Semantic Interpretation
TOON-AI Semantic Egnine
L2
Signal
Ambient confidence

JSON-AI Evidence Engine

Patient Alert
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Troponin I
0.8 ng/mL ↑
BNP
420 pg/mL ↑
HIGH
94% Confidence
Pattern recognition: Troponin elevation (baseline 0.02→0.8) combined with BNP rise (180→420) over 6hrs. Correlates with EKG changes at 02:34. Rule: biomarker_velocity + temporal_clustering → alert_priority_high
Evidence Trail

Source Record
Lab_2026-02-12_0834
HIPAA Encrypted Deep-link

L3
Rationale
Reasoning Path
TOON-AI Semantic Egnine
L4
Evidence
Source Attribution
JSON-AI Evidence Engine
JSON-AI (Evidence Engine)
TOON-AI (Semantic + Logic)
Core Flow Walkthrough
Interaction Map & Progressive Disclosure
Progressive disclosure: from ambient awareness to clinical decision
Two UI patterns: Continuity Strip (State 1-3) and Tieline Navigation (State 4)
State 1
Passive
The Glance
None
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
State 2
300ms Hover
The Lean-In (Dwell)
Hover
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
L3
Medication Discrepancy
Critical
Confidence: 94%
Metformin 1000mg BID found in CVS community record (filled 02/10), but missing from Epic chart. Patient reported taking medication during intake.
View Details
State 3
Click
The Audit (Action)
Click to expand
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
Medication Discrepancy Analysis
Evidence Deep-Dive
Source Comparison
Epic (Current)
No Metformin recorded
CVS Record
Metformin 1000mg BID
Filled: 02/10/2026
L4
Confidence: 94%

CVS_RX_2026-10_08:34:22
Prescription filled by Pharmacy ID: CVS-2847
Patient_Intake_2026-02-13_07:12:03
Verbal confirmation during admission
Epic_MedRec_Last_Updated_0225-11-03
Verbal confirmation during admission
Clinical Decision
Reconcile to Chart
Dismiss Alert
HIPAA Encrypted Deep-link
Continuity Strip: Progressive Disclosure
1
Passive Awareness
Ambient signals require zero cognitive load. Visual pulse communicates importance without interrupting workflows
2
contextual Insight
300ms dwell threshold reveals reasoning. Just-in-time information prevents alert fatigue while maintaining transparency
3
Verifiable Action
Full audit trail with clinical handshake. Every decision is traceable, reversible, and compliant with regulatory requirements
Shared Timeline
This isn’t a dashboard. It’s system memory
Why it exists
- Shift handoffs
- End-of-day review
- Cross-role reconciliation
What it shows
- Decisions and overrides
- AI insights with confidence
- Evidence trails across time
Systems Impact
Measuring Success
Validating continuity without increasing risk
What I’d Measure
Time to orientation
How quickly users understand what changed and what matters
Clarification loops
Back-and-forth caused by missing or unclear context
Scheduling failures
Downstream breakdowns caused by incomplete handoffs
AI insights acceptance vs override rates
A proxy for trust and signal quality
What I’d Test
- Confidence threshold tuning
- Role-based prioritization of insights
- Signal fatigue over time
Design Principle
AI earns trust by reducing work, not by demanding belief
Risks & Open Questions
Designing AI for real-world systems, not ideal conditions
Human Reality
- Trust must be earned
- Workflow disruption causes rejection
- Training and change fatigue are real
Integration Reality
- Varying EMR capabilities
- Limited control over host UI
- Long enterprise deployment cycles
Data Reality
- Incomplete records
- conflicting sources
- delayed or stale inputs
Design Responses & Mitigations


Core








Low Risk
Sidecar architeture
(low integration risk)




















Alert


Info
Visual separation from system alerts











CTRL

Explicit human confirmation and override
Let’s Work Together
Interested in collaborating on complex UI/UX challenges involving data, AI, or enterprise systems?
I’d love to explore how thoughtful design can drive clarity and business impact.

Get In Touch

About Kelli
Product Designer | AI x Data Systems
Passionate about turning complex data and AI systems into clear, trustworthy, human-centered experiences
Based in: San Francisco, CA
© 2026 Kelli Nordfelt
Overview
Problem
Tech Wall

Design
Impact
Retrospective
Overview
Designing AI Continuity in High Stakes Systems
Healthcare workflows break not because of a lack of data. They break because context doesn’t survive transitions.
Problem Framing
Stabilize Continuity • Predictive Reasoning • Not Automate Decisions
Why This Matters
Recent research highlights the importance of understanding patient state over time, not just at isolated moments.
MIRA: A Medical Foundation Model (NeurIPS)
Explores longitudinal modeling of medical data to enable more holistic insights across conditions.
This project applies that insight at the workflow level:
How continuity can be preserved across roles, systems, and handoffs without replacing human judgment.
The Hero Problem
Clinical continuity breaks across role boundaries and system transitions, forcing humans to rebuild context manually
High Cognitive Load • Repeated Work • Trust Gaps in AI tools
5 Day Product Design Sprint – From Discovery to Prototype
From scattered point points to a shared systemic problem
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
Problem Locked
Concept Selected
Prototype Ready
Objectives
Problem Framing
Analyze Current State
Ideate & Select
Build Prototype
Present & Plan
Research
& Discovery
Analyze current state
Synthesis
Current-State Mapping
Systems
& Design Thinking
Failure Analysis
AI Opportunity Framing
Prototyping
Low-fidelity flows
Core Flow Prototype
Persona Summaries
Final Narrative & Metrics
Deliverables
Workflow Diagram
Low-Fi Screens
Rapid Prototypes
The Problem & Discovery
Mapping the Shared Reality
From Retrieval to Proactive Delivery – The AI Layer
Identifying how Nurses, Physicians, and Specialists interact with data during crisis moments
Discovery & Interviews
Who I Spoke With
- Child & Adolescent Psychiatrist
- OB/GYN
- Maternal Fetal Medicine Physician (MFM)
- Registered Nurse (RN)
- Registration / Admin
What I Listened For
- Handoffs
- Cognitive load
- Risk points
- Trust boundaries
- AI adoption barriers
Physicians
“So many of our decisions are time-sensitive, but the information we need is often incomplete or scattered. I’m constantly double-checking because I don’t trust that I’m seeing the full picture.”
Breaks Today
Fragmented context, repeated documentation, low trust in prior data
Needs
Clear deltas, confidence-scored risks, evidence with human override
Nurses
“I’m interrupted constantly. I rely on quick signals to know what actually matters right now, but I still end up manually checking charts to make sure nothing critical was missed.”
Breaks Today
Interruptions, alert overload, manual safety checks
Needs
Prioritized tasks, trend signals, shift-safe handoffs
Admins
“When information is missing or changes without warning, we’re the ones trying to fix it. A small data issue upstream can turn into scheduling failures and patient frustration.”
Breaks Today
Missing context, silent automation failures, unclear urgency
Needs
Early risk signals, dependency visibility, auditable fixes
Emerging Themes & Cross-role Patterns
This validated continuity as a systemic problem, not UI issues
- Timing-sensitive decisions with incomplete data
- AI tools that help in isolation, but don’t connect the system
- Manual verification loops
- Repeated documentation
- Context loss at handoffs
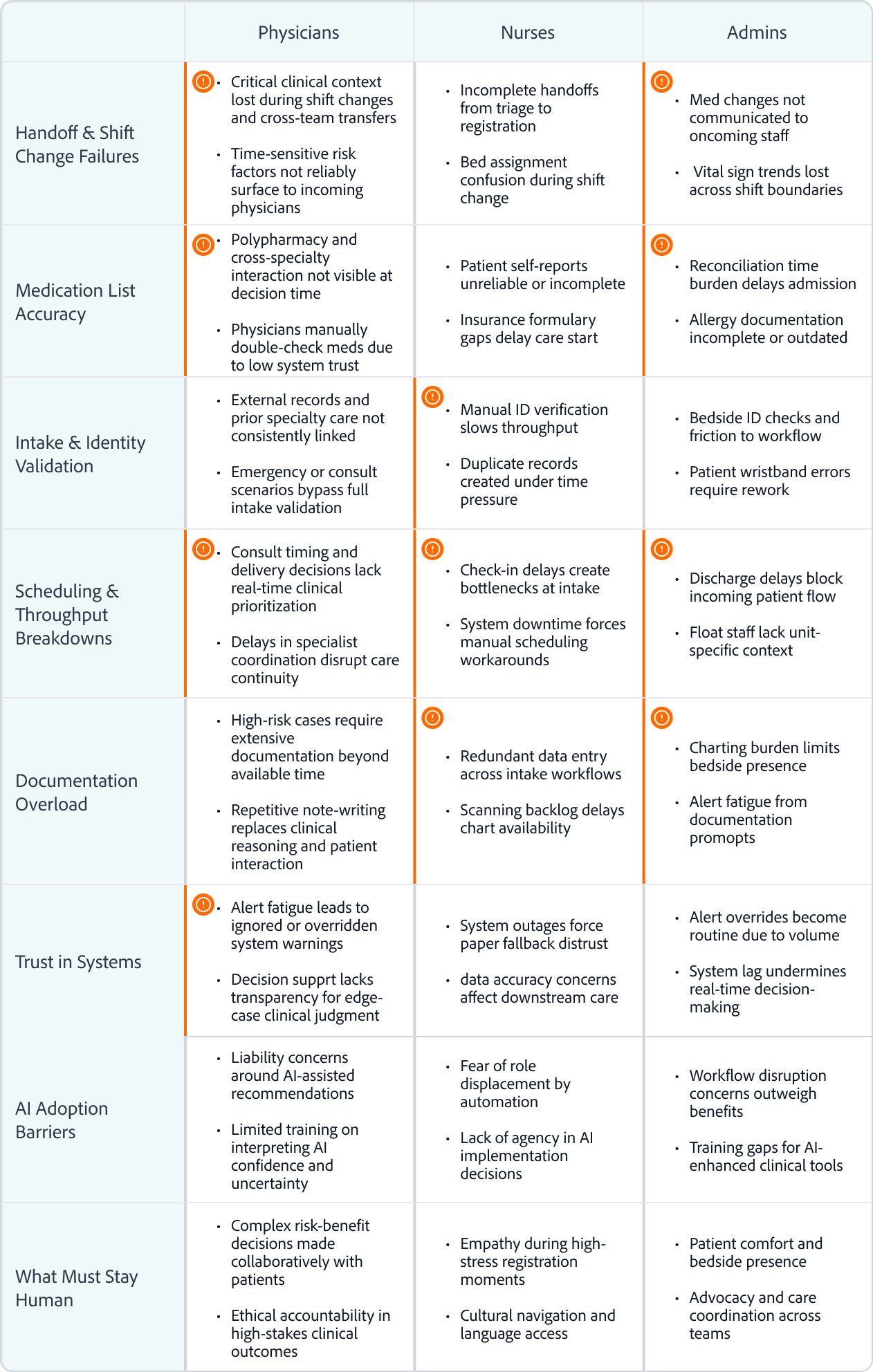
Emerging Problem Themes Across the Clinical Continuity Ecosystem
Patterns observed across clinicians, operations, and frontline care during discovery interviews
High-risk convergence across roles
Localized role friction
Physicians
Nurses
Admins
Handoff & Shift Change Failures

- Critical clinical context lost during shift changes and cross-team transfers
- Time-sensitive risk factors not reliably surface to incoming physicians
- Incomplete handoffs from triage to registration
- Bed assignment confusion during shift change
- Med changes not communicated to oncoming staff
- Vital sign trends lost across shift boundaries
Medication List Accuracy
- Polypharmacy and cross-specialty interaction not visible at decision time
- Physicians manually double-check meds due to low system trust
- Patient self-reports unreliable or incomplete
- Insurance formulary gaps delay care start
- Reconciliation time burden delays admission
- Allergy documentation incomplete or outdated
Intake & Identity Validation
- External records and prior specialty care not consistently linked
- Emergency or consult scenarios bypass full intake validation
- Manual ID verification slows throughput
- Duplicate records created under time pressure
- Bedside ID checks and friction to workflow
- Patient wristband errors require rework
Scheduling & Throughput Breakdowns
- Consult timing and delivery decisions lack real-time clinical prioritization
- Delays in specialist coordination disrupt care continuity
- Check-in delays create bottlenecks at intake
- System downtime forces manual scheduling workarounds
- Discharge delays block incoming patient flow
- Float staff lack unit-specific context
Documentation Overload
- High-risk cases require extensive documentation beyond available time
- Repetitive note-writing replaces clinical reasoning and patient interaction
- Redundant data entry across intake workflows
- Scanning backlog delays chart availability
- Charting burden limits bedside presence
- Alert fatigue from documentation promopts
Trust in Systems
- Alert fatigue leads to ignored or overridden system warnings
- Decision supprt lacks transparency for edge-case clinical judgment
- System outages force paper fallback distrust
- data accuracy concerns affect downstream care
- Alert overrides become routine due to volume
- System lag undermines real-time decision-making
AI Adoption Barriers
- Liability concerns around AI-assisted recommendations
- Limited training on interpreting AI confidence and uncertainty
- Fear of role displacement by automation
- Lack of agency in AI implementation decisions
- Workflow disruption concerns outweigh benefits
- Training gaps for AI-enhanced clinical tools
What Must Stay Human
- Complex risk-benefit decisions made collaboratively with patients
- Ethical accountability in high-stakes clinical outcomes
- Empathy during high-stress registration moments
- Cultural navigation and language access
- Patient comfort and bedside presence
- Advocacy and care coordination across teams
The Technical Wall
From Retrieval to Proactive Context
Why clinicians are forced to rebuild context by hand
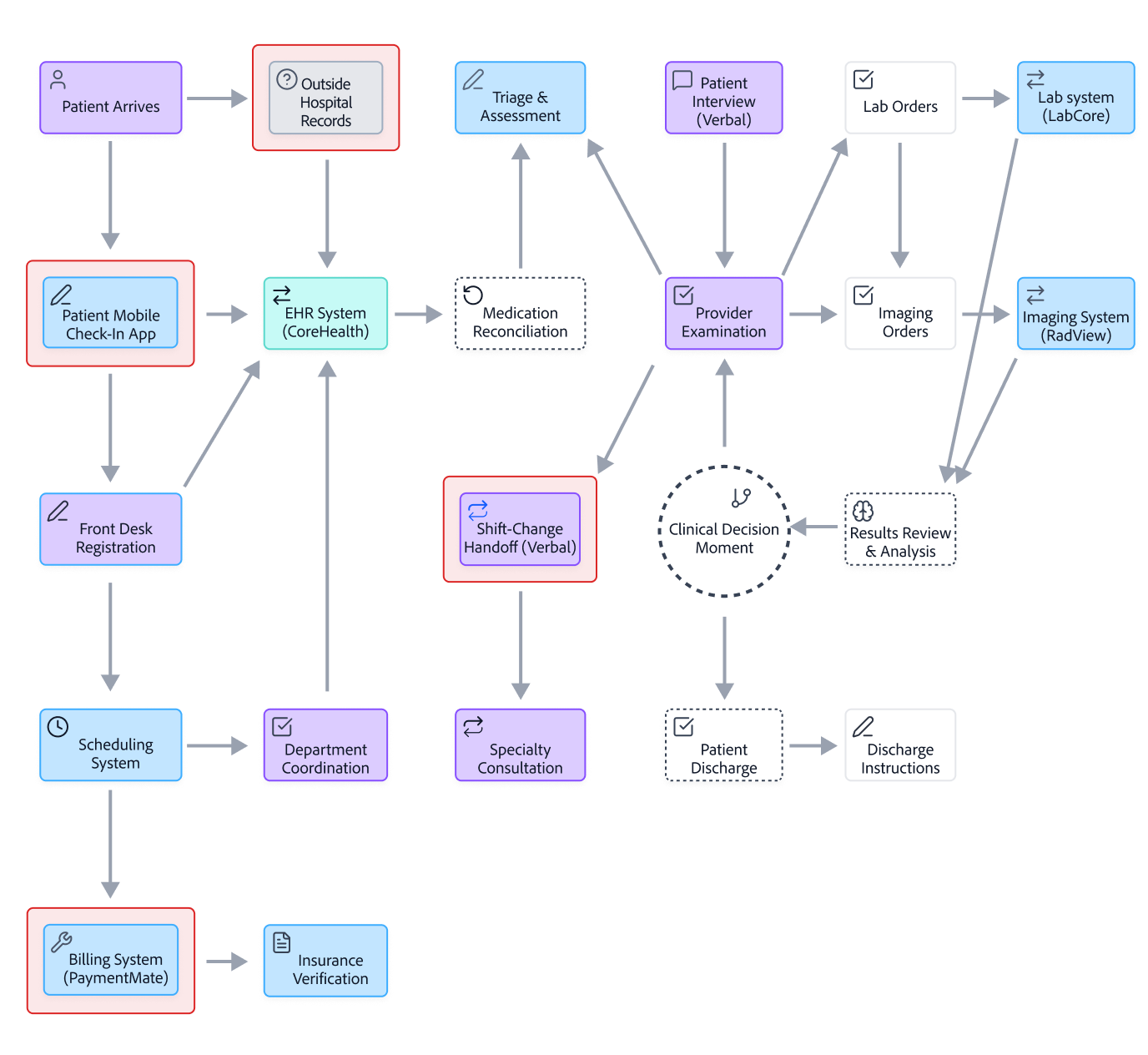
Current-State Clinical Workflow: Fragmented Continuity of Care
Where Fragmentation, Repetition, and Trust Gaps Occur
Human Input
Decision Moment
Operational Systems
External Sources
EHR System (CoreHealth)
Info Artifact
View Failure Points

Provider
Examination
Imaging Orders
Lab Orders
Clinical Decision Moment


Triage & Assessment

Results Review
& Analysis




Insurance Verification




EHR System
(CoreHealth)




Lab system
(LabCore)

Outside
Hospital Records

Patient Interview
(Verbal)

Patient Arrives

Patient Mobile
Check-In App
Front Desk Registration

Scheduling System

Billing System
(PaymentMate)
Department Coordination

Specialty
Consultation
Patient
Discharge
Discharge Instructions
Imaging System
(RadView)

Shift-Change
Handoff (Verbal)

Medication
Reconciliation
















7
Human Touchpoint’s
(Many-to-Many Communication Load)
4
External Data Sources
(Many-to-Many Fragmentation Risk)
4
High-Stakes
Decision Moments
1
Central EHR Record
(Single Source of Truth, Limited Context)
7
Operational Systems per Patient Journey
(1-to-Many Integration Burden)
Fragmented Inputs Create Hidden Clinical Risk
Care teams must coordinate across multiple human handoffs, disconnected operational systems, and incomplete external records. The EHR acts as a central hub, but critical context remains distributed, forcing clinicians to bridge gaps manually during high-stakes decision moments.
AI Opportunity Framework
Two complementary AI Layers Working Together
JSON-AI Layer
(Structured Intelligence)
Structured continuity intelligence
- Medication reconciliation
- Scheduling logic & insurance verification
- Clean summaries
- Continuity “checklist” generation
TOON-AI Layer
(Narrative/Reasoning AI)
Interpretive reasoning
- Nuance-finding in handoffs
- Rick deltas
- Inconsistencies in the patient story
- Reasoning across notes and conversations
- Role-specific briefings
AI restores context so human judgment can be used with confidence
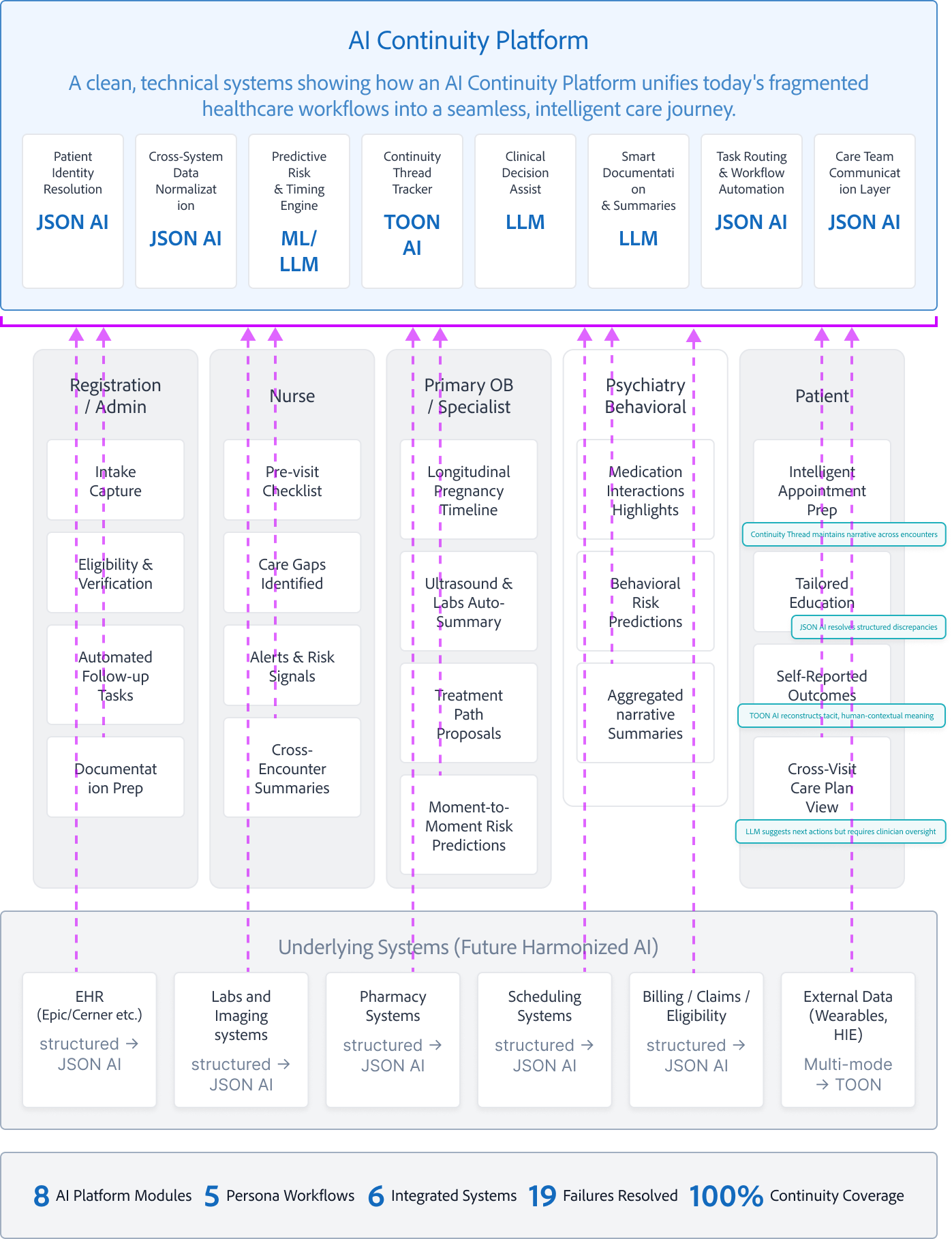
Future-State: AI Continuity Platform Across the Care Journey
A clean, technical systems diagram showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
AI Continuity Platform
A clean, technical systems showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
Patient
Identity Resolution
JSON AI
Cross-System Data Normalization
JSON AI
Predictive Risk
& Timing Engine
ML/LLM
Continuity
Thread Tracker
TOON AI
Clinical
Decision Assist
LLM
Smart Documentation
& Summaries
LLM
Task Routing & Workflow Automation
JSON AI
Care Team
Communication Layer
JSON AI
Registration / Admin
Intake Capture
Eligibility & Verification
Automated Follow-up Tasks
Documentation Prep
Nurse
Pre-visit Checklist
Care Gaps Identified
Alerts & Risk Signals
Cross-Encounter Summaries
Primary OB / Specialist
Longitudinal Pregnancy Timeline
Ultrasound & Labs Auto-Summary
Treatment Path Proposals
Moment-to-Moment Risk Predictions
Psychiatry Behavioral
Medication Interactions Highlights
Behavioral Risk Predictions
Aggregated narrative Summaries
Patient
Intelligent Appointment Prep
Tailored Education
Self-Reported Outcomes
Cross-Visit Care Plan View
Continuity Thread maintains narrative across encounters
JSON AI resolves structured discrepancies
TOON AI reconstructs tacit, human-contextual meaning
LLM suggests next actions but requires clinician oversight
Underlying Systems (Future Harmonized AI)
EHR (Epic/Cerner etc.)
structured → JSON AI
Labs and Imaging systems
structured → JSON AI
Pharmacy Systems
structured → JSON AI
Scheduling Systems
structured → JSON AI
Billing / Claims / Eligibility
structured → JSON AI
External Data
(Wearables, HIE)
Multi-mode → TOON






8
AI Platform Modules
5
Persona Workflows
6
Integrated Systems
19
Failures Resolved
100%
Continuity Coverage
Design Pivot
Designing the Clinical
Intelligence Layer
Different surfaces. Same continuity intelligence
Continuity cannot live in a single interface. It must persist across roles, tools, and time
Three Patterns for AI-Supported Continuity
To avoid “Dashboard Fatigue,” we can move explainability to the object level. Each insight adapts to the persona while utilizing three core patterns.
Continuity Strip
- Explainable, cross-system, non-blocking
- Persistent continuity without competing with system alerts
Sidecar Panel
- System memory across roles and time
- Handoffs, overrides, and reasoning in one place
Shared Timeline
- Moment-of-decision context
- What changed, what matters now, What is next
Persona-Specific Workflows
AI utility is not one-size-fits-all
The system surfaces the same “Intelligence Object” in different formats depending on the user’s role” Physicians receive deep-dive rationale for diagnosis, Nurses see actionable safety threads during handoff, and Admins receive operational status updates to clear discharge bottlenecks.
One Critical Event, Three Interpretations
An external record from St. Mary’s Hospital arrives at 08:42 AM, revealing HIGH-RISK PENICILLIN ALLERGY not documented in the Epic chart. The AI detects this discrepancy and surfaces it differently for each decision owner’s specific pressure points.
Dr. Aris Chen
Attending Physician
Primary Goal
Validate diagnostic risk & maintain accuracy
Decision Pressure Points:
- Deep work mode, cannot tolerate interruptions
- Needs full evidence trail for liability
- Must understand "why" before acting
UI Pattern: The Sidecar Panel
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
AI Continuity
Context for this shift
Patient Insights
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Evidence Trail
St. Mary’s discharge summary (02/10) • Confirmed via FHIR import • Verified anaphylaxis history
The Clinical Handshake:
Verify & Update Chart
Flag as Error
Human remains final authority. Action logged to audit trail.
Sarah Martinez, RN
Charge Nurse
Primary Goal
Execute safe tasks during handoff
Decision Pressure Points:
- High task density—needs glanceable safety checks
- Shift handoff = critical error window
- Must act fast without missing context
UI Pattern: The Shared Timeline
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.

Medication Administration
Scheduled Administration
10:00
Amoxicillin 500mg PO
ALLERGY CONFLICT
Critical
Penicillin allergy detected in external record. Amoxicillin is contraindicated.
HIGH
94% Confidence
Auto-flagged
Scheduled assessment
14:00
Amoxicillin 500mg PO
The Clinical Handshake:
Hold Medication
Page Provider
Error prevented. Intervention escalated to physician.
Marcus Kim
Care Coordinator
Primary Goal
Clear discharge bottlenecks & ensure compliance
Decision Pressure Points:
- Manages 40+ patients and needs status at-a-glance
- Doesn’t need clinical PII< just completion status
- Discharge delays = throughput bottlenecks
UI Pattern: Exception-Based Alert Feed
No dashboard to monitor. System PUSHES critical blockers to the feed. Silent when everything flows smoothly.
Active Discharge Blocker Detected
Patient 847-2931
Ready
Patient 847-2931
✓ Now Complete
Status Update
Critical data gap resolved at 08:47
Allergy record reconciled & verified
Patient 847-2931
Pending...
The Clinical Handshake:
Mark Discharge-Ready
View Full Feed
Bottleneck cleared. Patient ready for discharge workflow.
The Clinical Handshake: Closing the Loop
Regardless of role, every interaction ends in a HANDSHAKE. A deliberate human action that confirms or rejects the AI’s synthesis. This ensures that while the AI handles the data plumbing, the human remains the final authority in the clinical record.
Physician
Verify & update with full audit trail
Nurse
Hold medication & escalate to provider
Admin
Mark complete & clear bottleneck
Structural Evolution
From fragmented workspaces to AI-curated chronology
Before
Fragmented Workspaces
TAB CHAOS
Patient
Labs
Med Rec
+8
Verbal Note (Tab 1)
“Patient reports taking Metformin...”
Nurse intake 02/13
Outside PDF (Tab 3)
St. Mary's Hospital Discharge Summary
Scanned: 01/10/2026
Lab Result (Tab 2)
Troponin: 0.8 ng/mL
01/12/2026 13:34
Med Rec (Tab 4)
“Patient reports taking Metformin...”
103 days old

Manual
Integration
After
AI-Curated Timeline
UNIFIED CHRONOLOGY
Shared Timeline
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Outside Hospital Discharge
02/10/ 14:22
St. Mary’s Hospital • Cardiac Event
JSON-AI auto-parsed PDF
Matched: Discharge RX → Pharmacy
Pharmacy Fill
Metformin 1000mg BID • CVS Pharmacy
TOON-AI linked to discharge orders
02/10/ 16:45
Verified: Nurse note ↔ Pharmacy
Lab Result Anomaly
Troponin I: 0.8 ng/mL ↑ (Critical)
JSON-AI flagged spike pattern
02/12/ 08:34
Linked: Cardiac event → Lab spike
Intake Verification
Nurse confirmed Metformin use verbally
TOON-AI reconciled with CVS record
02/13/ 07:12
Matched: Discharge RX → Parmacy
AI-Insight
Med discrepancy + cardiac markers = High-risk patterns
Now
HIGH
94% Confidence
Auto-flagged before first dose
The Clinical Handshake: Closing the Loop
Problem
Data fragmentation forces clinicians to become “human middleware,” manually integrating disparate sources.
Solution
AI becomes the integration layer, automatically reconciling cross-system data into a unified temporal model.
Impact
Clinicians focus on care decisions, not data archeaology. Critical patterns emerge from temporal synthesis
Action vs. Priority
Preventing Compliance Fatigue
In high-stakes systems, you must distinguish between Actionable Intelligence and Critical Awareness
If you force an "Action" on everything that is "High Priority," you create a "Compliance UI" where users click "OK" just to clear the screen—which is how major medical errors happen.
The Compliance Fatigue Problem
Traditional alert systems conflate Priority (clinical urgency) with Action Required (system needs input). This creates alert fatigue where clinicians dismiss critical warnings just to continue working, leading to preventable medical errors.
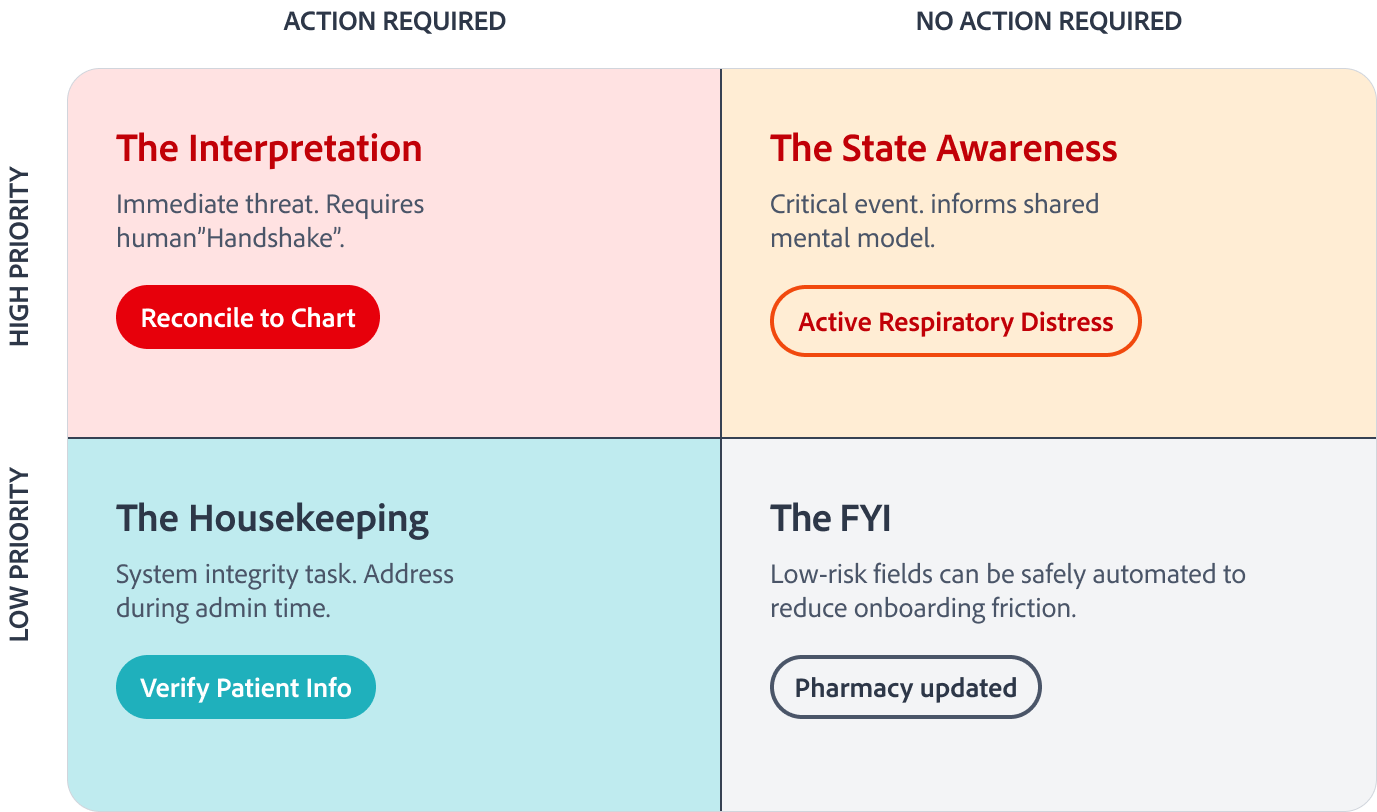
Intelligence Action Taxonomy Matrix
Decoupling Action from Urgency
HIGH PRIORITY
LOW PRIORITY
ACTION REQUIRED
NO ACTION REQUIRED
The Interpretation
Immediate threat. Requires human”Handshake”.
Reconcile to Chart
The State Awareness
Critical event. informs shared mental model.
Active Respiratory Distress
The FYI
Low-risk fields can be safely automated to reduce onboarding friction.
Pharmacy updated
The Housekeeping
System integrity task. Address during admin time.
Verify Patient Info
Timeline Visual System
Multimodal Encoding
Progressive disclosure through three-stage scaling and verification state encoding
Icons are hard to see in passive timeline views. This system maintains clarity without cluttering the screen through intelligent scale transitions and semantic color+glyph pairing.
Three-Stage Scaling Strategy
Progressive visual complexity based on user engagement level
16px
Stage 1: Passive
Small dot only. No icon. Keeps the "spine" clean for scrolling through long timelines. Low cognitive load.
32px on hover
Stage 2: Focus
On hover/scroll proximity, node expands to 16px and white glyph fades in. The "Aha!" moment where category is confirmed.
L1: Medication Order
L2: Verified by clinician
02/12 14:08
24px icon in card header
Stage 3: Object
Inside Intel Object Card, icon appears at 24px next to L1 Signal text. Full context revealed.
Why These Patterns
Tradeoffs Under Real-world Constraints
Patterns were selected to fit real systems, not idealized workflows
These patterns were chosen to:
- Respect existing systems of record
- Work across multiple environments
- Minimize workflow disruption
- Allow trust to build incrementally
Why not dashboards?
They centralize information but pull users out of real workflows.
Why not alerts everywhere?
They compete with native warnings and accelerate alert fatigue.
Why not overlays by default?
They interrupt primary tasks and don’t scale across systems.
Structural Evolution
From fragmented workspaces to AI-curated chronology
Anatomy of a Clinical Intelligence Object
A four-layer metadata hierarchy ensuring explainability through Signal,Insight, Rationale, and Evidence
Insight
L1
Semantic Interpretation
Semantic synthesis generated by TOON-AI. Natural language interpretation transforms raw clinical data into actionable intelligence.
TOON-AI Semantic Engine
Signal
L2
Ambient confidence
Confidence Score mapped to opacity pulse. Visual indicator provides immediate ambient awareness of data reliability without cognitive overhead.
JSON-AI Evidence Engine
Patient Alert
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Troponin I
0.8 ng/mL ↑
BNP
420 pg/mL ↑
HIGH 94% Confidence details
Pattern recognition: Troponin elevation (baseline 0.02→0.8) combined with BNP rise (180→420) over 6hrs. Correlates with EKG changes at 02:34. Rule: biomarker_velocity + temporal_clustering → alert_priority_high
Evidence Trail
Source Record
Lab_2026-02-12_0834
HIPAA Encrypted Deep-link

L3
Rationale
Reasoning Path
Hidden behind hover/dwell interaction to reduce visual noise. Reveals the computational logic and decision tree that led to this insight, maintaining transparency without overwhelming the interface
TOON-AI Semantic Engine
L4
Evidence
Source Attribution
Direct deep-link to source EHR record with HIPAA encryption. Enables immediate audit trail and source verification, critical for clinical decision support and regularity compliance.
JSON-AI Evidence Engine
JSON-AI (Evidence Engine)
TOON-AI (Semantic + Logic)
Core Flow Walkthrough
Interaction Map & Progressive Disclosure
Progressive disclosure: from ambient awareness to clinical decision
Two UI patterns: Continuity Strip (State 1-3) and Tieline Navigation (State 4)
State 1
Passive
The Glance
None
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
State 2
300ms Hover
The Lean-In (Dwell)
Hover
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
L3
Medication Discrepancy
Critical
Confidence: 94%
Metformin 1000mg BID found in CVS community record (filled 02/10), but missing from Epic chart. Patient reported taking medication during intake.
View Details
State 3
Click
The Audit (Action)
Click to expand
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
Medication Discrepancy Analysis
Evidence Deep-Dive
Source Comparison
Epic (Current)
No Metformin recorded
CVS Record
Metformin 1000mg BID
Filled: 02/10/2026
L4
Confidence: 94%
CVS_RX_2026-10_08:34:22
Prescription filled by Pharmacy ID: CVS-2847
Patient_Intake_2026-02-13_07:12:03
Verbal confirmation during admission
Epic_MedRec_Last_Updated_0225-11-03
Verbal confirmation during admission
Clinical Decision
Reconcile to Chart
Dismiss Alert
HIPAA Encrypted Deep-link
Continuity Strip: Progressive Disclosure
1
Passive Awareness
Ambient signals require zero cognitive load. Visual pulse communicates importance without interrupting workflows
2
contextual Insight
300ms dwell threshold reveals reasoning. Just-in-time information prevents alert fatigue while maintaining transparency
3
Verifiable Action
Full audit trail with clinical handshake. Every decision is traceable, reversible, and compliant with regulatory requirements
Shared Timeline
This isn’t a dashboard. It’s system memory
Why it exists
- Shift handoffs
- End-of-day review
- Cross-role reconciliation
What it shows
- Decisions and overrides
- AI insights with confidence
- Evidence trails across time
Systems Impact
Measuring Success
Validating continuity without increasing risk
What I’d Measure
Time to orientation
How quickly users understand what changed and what matters
Clarification loops
Back-and-forth caused by missing or unclear context
Scheduling failures
Downstream breakdowns caused by incomplete handoffs
AI insights acceptance vs override rates
A proxy for trust and signal quality
What I’d Test
- Confidence threshold tuning
- Role-based prioritization of insights
- Signal fatigue over time
Design Principle
AI earns trust by reducing work, not by demanding belief
Risks & Open Questions
Designing AI for real-world systems, not ideal conditions
Human Reality
- Trust must be earned
- Workflow disruption causes rejection
- Training and change fatigue are real
Integration Reality
- Varying EMR capabilities
- Limited control over host UI
- Long enterprise deployment cycles
Data Reality
- Incomplete records
- conflicting sources
- delayed or stale inputs
Design Responses & Mitigations
Core
Low Risk
Sidecar architeture
(low integration risk)
Alert
Info
Visual separation from system alerts
CTRL
Explicit human confirmation and override
Let’s Work Together
Interested in collaborating on complex UI/UX challenges involving data, AI, or enterprise systems?
I’d love to explore how thoughtful design can drive clarity and business impact.
Get In Touch
About Kelli
Product Designer | AI x Data Systems
Passionate about turning complex data and AI systems into clear, trustworthy, human-centered experiences
Based in: San Francisco, CA
© 2026 Kelli Nordfelt
Overview
Designing AI Continuity in High Stakes Systems
Healthcare workflows break not because of a lack of data. They break because context doesn’t survive transitions.
Problem Framing
Stabilize Continuity • Predictive Reasoning • Not Automate Decisions
Why This Matters
Recent research highlights the importance of understanding patient state over time, not just at isolated moments.
MIRA: A Medical Foundation Model (NeurIPS)
Explores longitudinal modeling of medical data to enable more holistic insights across conditions.
This project applies that insight at the workflow level:
How continuity can be preserved across roles, systems, and handoffs without replacing human judgment.
The Hero Problem
Clinical continuity breaks across role boundaries and system transitions, forcing humans to rebuild context manually
High Cognitive Load • Repeated Work • Trust Gaps in AI tools
5 Day Product Design Sprint – From Discovery to Prototype
From scattered point points to a shared systemic problem
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
Problem Locked
Concept Selected
Prototype Ready
Objectives
Problem Framing
Analyze Current State
Ideate & Select
Build Prototype
Present & Plan
Research
& Discovery
Analyze current state
Synthesis
Current-State Mapping
Systems
& Design Thinking
Failure Analysis
AI Opportunity Framing
Prototyping
Low-fidelity flows
Core Flow Prototype
Persona Summaries
Final Narrative & Metrics
Deliverables
Workflow Diagram
Low-Fi Screens
Rapid Prototypes
The Problem & Discovery
Mapping the Shared Reality
From Retrieval to Proactive Delivery – The AI Layer
Identifying how Nurses, Physicians, and Specialists interact with data during crisis moments
Discovery & Interviews
Who I Spoke With
- Child & Adolescent Psychiatrist
- OB/GYN
- Maternal Fetal Medicine Physician (MFM)
- Registered Nurse (RN)
- Registration / Admin
What I Listened For
- Handoffs
- Cognitive load
- Risk points
- Trust boundaries
- AI adoption barriers
Physicians
“So many of our decisions are time-sensitive, but the information we need is often incomplete or scattered. I’m constantly double-checking because I don’t trust that I’m seeing the full picture.”
Breaks Today
Fragmented context, repeated documentation, low trust in prior data
Needs
Clear deltas, confidence-scored risks, evidence with human override
Nurses
“I’m interrupted constantly. I rely on quick signals to know what actually matters right now, but I still end up manually checking charts to make sure nothing critical was missed.”
Breaks Today
Interruptions, alert overload, manual safety checks
Needs
Prioritized tasks, trend signals, shift-safe handoffs
Admins
“When information is missing or changes without warning, we’re the ones trying to fix it. A small data issue upstream can turn into scheduling failures and patient frustration.”
Breaks Today
Missing context, silent automation failures, unclear urgency
Needs
Early risk signals, dependency visibility, auditable fixes
Emerging Themes & Cross-role Patterns
This validated continuity as a systemic problem, not UI issues
- Timing-sensitive decisions with incomplete data
- AI tools that help in isolation, but don’t connect the system
- Manual verification loops
- Repeated documentation
- Context loss at handoffs
Emerging Problem Themes Across the Clinical Continuity Ecosystem
Patterns observed across clinicians, operations, and frontline care during discovery interviews
High-risk convergence across roles
Localized role friction
Physicians
Nurses
Admins
Handoff & Shift Change Failures
- Critical clinical context lost during shift changes and cross-team transfers
- Time-sensitive risk factors not reliably surface to incoming physicians
- Incomplete handoffs from triage to registration
- Bed assignment confusion during shift change
- Med changes not communicated to oncoming staff
- Vital sign trends lost across shift boundaries
Medication List Accuracy
- Polypharmacy and cross-specialty interaction not visible at decision time
- Physicians manually double-check meds due to low system trust
- Patient self-reports unreliable or incomplete
- Insurance formulary gaps delay care start
- Reconciliation time burden delays admission
- Allergy documentation incomplete or outdated
Intake & Identity Validation
- External records and prior specialty care not consistently linked
- Emergency or consult scenarios bypass full intake validation
- Manual ID verification slows throughput
- Duplicate records created under time pressure
- Bedside ID checks and friction to workflow
- Patient wristband errors require rework
Scheduling & Throughput Breakdowns
- Consult timing and delivery decisions lack real-time clinical prioritization
- Delays in specialist coordination disrupt care continuity
- Check-in delays create bottlenecks at intake
- System downtime forces manual scheduling workarounds
- Discharge delays block incoming patient flow
- Float staff lack unit-specific context
Documentation Overload
- High-risk cases require extensive documentation beyond available time
- Repetitive note-writing replaces clinical reasoning and patient interaction
- Redundant data entry across intake workflows
- Scanning backlog delays chart availability
- Charting burden limits bedside presence
- Alert fatigue from documentation promopts
Trust in Systems
- Alert fatigue leads to ignored or overridden system warnings
- Decision supprt lacks transparency for edge-case clinical judgment
- System outages force paper fallback distrust
- data accuracy concerns affect downstream care
- Alert overrides become routine due to volume
- System lag undermines real-time decision-making
AI Adoption Barriers
- Liability concerns around AI-assisted recommendations
- Limited training on interpreting AI confidence and uncertainty
- Fear of role displacement by automation
- Lack of agency in AI implementation decisions
- Workflow disruption concerns outweigh benefits
- Training gaps for AI-enhanced clinical tools
What Must Stay Human
- Complex risk-benefit decisions made collaboratively with patients
- Ethical accountability in high-stakes clinical outcomes
- Empathy during high-stress registration moments
- Cultural navigation and language access
- Patient comfort and bedside presence
- Advocacy and care coordination across teams
The Technical Wall
From Retrieval to Proactive Context
Why clinicians are forced to rebuild context by hand
Current-State Clinical Workflow: Fragmented Continuity of Care
Where Fragmentation, Repetition, and Trust Gaps Occur
Human Input
Decision Moment
Operational Systems
External Sources
EHR System (CoreHealth)
Info Artifact
View Failure Points
Provider
Examination
Imaging Orders
Lab Orders
Clinical Decision Moment
Triage & Assessment
Results Review
& Analysis
Insurance Verification
EHR System
(CoreHealth)
Lab system
(LabCore)
Outside
Hospital Records
Patient Interview
(Verbal)
Patient Arrives
Patient Mobile
Check-In App
Front Desk Registration
Scheduling System
Billing System
(PaymentMate)
Department Coordination
Specialty
Consultation
Patient
Discharge
Discharge Instructions
Imaging System
(RadView)
Shift-Change
Handoff (Verbal)
Medication
Reconciliation
















7
Human Touchpoint’s
(Many-to-Many Communication Load)
4
External Data Sources
(Many-to-Many Fragmentation Risk)
4
High-Stakes
Decision Moments
1
Central EHR Record
(Single Source of Truth, Limited Context)
7
Operational Systems per Patient Journey
(1-to-Many Integration Burden)
Fragmented Inputs Create Hidden Clinical Risk
Care teams must coordinate across multiple human handoffs, disconnected operational systems, and incomplete external records. The EHR acts as a central hub, but critical context remains distributed, forcing clinicians to bridge gaps manually during high-stakes decision moments.
AI Opportunity Framework
Two complementary AI Layers Working Together
JSON-AI Layer
(Structured Intelligence)
Structured continuity intelligence
- Medication reconciliation
- Scheduling logic & insurance verification
- Clean summaries
- Continuity “checklist” generation
TOON-AI Layer
(Narrative/Reasoning AI)
Interpretive reasoning
- Nuance-finding in handoffs
- Rick deltas
- Inconsistencies in the patient story
- Reasoning across notes and conversations
- Role-specific briefings
AI restores context so human judgment can be used with confidence
Future-State: AI Continuity Platform Across the Care Journey
A clean, technical systems diagram showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
AI Continuity Platform
A clean, technical systems showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
Patient
Identity Resolution
JSON AI
Cross-System Data Normalization
JSON AI
Predictive Risk
& Timing Engine
ML/LLM
Continuity
Thread Tracker
TOON AI
Clinical
Decision Assist
LLM
Smart Documentation
& Summaries
LLM
Task Routing & Workflow Automation
JSON AI
Care Team
Communication Layer
JSON AI
Registration / Admin
Intake Capture
Eligibility & Verification
Automated Follow-up Tasks
Documentation Prep
Nurse
Pre-visit Checklist
Care Gaps Identified
Alerts & Risk Signals
Cross-Encounter Summaries
Primary OB / Specialist
Longitudinal Pregnancy Timeline
Ultrasound & Labs Auto-Summary
Treatment Path Proposals
Moment-to-Moment Risk Predictions
Psychiatry Behavioral
Medication Interactions Highlights
Behavioral Risk Predictions
Aggregated narrative Summaries
Patient
Intelligent Appointment Prep
Tailored Education
Self-Reported Outcomes
Cross-Visit Care Plan View
Continuity Thread maintains narrative across encounters
JSON AI resolves structured discrepancies
TOON AI reconstructs tacit, human-contextual meaning
LLM suggests next actions but requires clinician oversight
Underlying Systems (Future Harmonized AI)
EHR (Epic/Cerner etc.)
structured → JSON AI
Labs and Imaging systems
structured → JSON AI
Pharmacy Systems
structured → JSON AI
Scheduling Systems
structured → JSON AI
Billing / Claims / Eligibility
structured → JSON AI
External Data
(Wearables, HIE)
Multi-mode → TOON






8
AI Platform Modules
5
Persona Workflows
6
Integrated Systems
19
Failures Resolved
100%
Continuity Coverage
Design Pivot
Designing the Clinical Intelligence Layer
Different surfaces. Same continuity intelligence
Continuity cannot live in a single interface. It must persist across roles, tools, and time
Three Patterns for AI-Supported Continuity
To avoid “Dashboard Fatigue,” we can move explainability to the object level. Each insight adapts to the persona while utilizing three core patterns.
Continuity Strip
- Explainable, cross-system, non-blocking
- Persistent continuity without competing with system alerts
Sidecar Panel
- System memory across roles and time
- Handoffs, overrides, and reasoning in one place
Shared Timeline
- Moment-of-decision context
- What changed, what matters now, What is next
Persona-Specific Workflows
AI utility is not one-size-fits-all
The system surfaces the same “Intelligence Object” in different formats depending on the user’s role” Physicians receive deep-dive rationale for diagnosis, Nurses see actionable safety threads during handoff, and Admins receive operational status updates to clear discharge bottlenecks.
One Critical Event, Three Interpretations
An external record from St. Mary’s Hospital arrives at 08:42 AM, revealing HIGH-RISK PENICILLIN ALLERGY not documented in the Epic chart. The AI detects this discrepancy and surfaces it differently for each decision owner’s specific pressure points.
Dr. Aris Chen
Attending Physician
Primary Goal
Validate diagnostic risk & maintain accuracy
Decision Pressure Points:
- Deep work mode, cannot tolerate interruptions
- Needs full evidence trail for liability
- Must understand "why" before acting
UI Pattern: The Sidecar Panel
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
AI Continuity
Context for this shift
Patient Insights
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Evidence Trail
St. Mary’s discharge summary (02/10) • Confirmed via FHIR import • Verified anaphylaxis history
The Clinical Handshake:
Verify & Update Chart
Flag as Error
Human remains final authority. Action logged to audit trail.
Sarah Martinez, RN
Charge Nurse
Primary Goal
Execute safe tasks during handoff
Decision Pressure Points:
- High task density—needs glanceable safety checks
- Shift handoff = critical error window
- Must act fast without missing context
UI Pattern: The Shared Timeline
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Medication Administration
Scheduled Administration
10:00
Amoxicillin 500mg PO
ALLERGY CONFLICT
Critical
Penicillin allergy detected in external record. Amoxicillin is contraindicated.
HIGH
94% Confidence
Auto-flagged
Scheduled assessment
14:00
Amoxicillin 500mg PO
The Clinical Handshake:
Hold Medication
Page Provider
Error prevented. Intervention escalated to physician.
Marcus Kim
Care Coordinator
Primary Goal
Clear discharge bottlenecks & ensure compliance
Decision Pressure Points:
- Manages 40+ patients and needs status at-a-glance
- Doesn’t need clinical PII< just completion status
- Discharge delays = throughput bottlenecks
UI Pattern: Exception-Based Alert Feed
No dashboard to monitor. System PUSHES critical blockers to the feed. Silent when everything flows smoothly.
Active Discharge Blocker Detected
Patient 847-2931
Ready
Patient 847-2931
✓ Now Complete
Status Update
Critical data gap resolved at 08:47
Allergy record reconciled & verified
Patient 847-2931
Pending...
The Clinical Handshake:
Mark Discharge-Ready
View Full Feed
Bottleneck cleared. Patient ready for discharge workflow.
The Clinical Handshake: Closing the Loop
Regardless of role, every interaction ends in a HANDSHAKE. A deliberate human action that confirms or rejects the AI’s synthesis. This ensures that while the AI handles the data plumbing, the human remains the final authority in the clinical record.
Physician
Verify & update with full audit trail
Nurse
Hold medication & escalate to provider
Admin
Mark complete & clear bottleneck
Structural Evolution
From fragmented workspaces to AI-curated chronology
Before
Fragmented Workspaces
TAB CHAOS
Patient
Labs
Med Rec
+8
Verbal Note (Tab 1)
“Patient reports taking Metformin...”
Nurse intake 02/13
Outside PDF (Tab 3)
St. Mary's Hospital Discharge Summary
Scanned: 01/10/2026
Lab Result (Tab 2)
Troponin: 0.8 ng/mL
01/12/2026 13:34
Med Rec (Tab 4)
“Patient reports taking Metformin...”
103 days old

Manual
Integration
After
AI-Curated Timeline
UNIFIED CHRONOLOGY
Shared Timeline
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Outside Hospital Discharge
02/10/ 14:22
St. Mary’s Hospital • Cardiac Event
JSON-AI auto-parsed PDF
Matched: Discharge RX → Pharmacy
Pharmacy Fill
Metformin 1000mg BID • CVS Pharmacy
TOON-AI linked to discharge orders
02/10/ 16:45
Verified: Nurse note ↔ Pharmacy
Lab Result Anomaly
Troponin I: 0.8 ng/mL ↑ (Critical)
JSON-AI flagged spike pattern
02/12/ 08:34
Linked: Cardiac event → Lab spike
Intake Verification
Nurse confirmed Metformin use verbally
TOON-AI reconciled with CVS record
02/13/ 07:12
Matched: Discharge RX → Parmacy
AI-Insight
Med discrepancy + cardiac markers = High-risk patterns
Now
HIGH
94% Confidence
Auto-flagged before first dose
The Clinical Handshake: Closing the Loop
Problem
Data fragmentation forces clinicians to become “human middleware,” manually integrating disparate sources.
Solution
AI becomes the integration layer, automatically reconciling cross-system data into a unified temporal model.
Impact
Clinicians focus on care decisions, not data archeaology. Critical patterns emerge from temporal synthesis
Action vs. Priority
Preventing Compliance Fatigue
In high-stakes systems, you must distinguish between Actionable Intelligence and Critical Awareness
If you force an "Action" on everything that is "High Priority," you create a "Compliance UI" where users click "OK" just to clear the screen—which is how major medical errors happen.
The Compliance Fatigue Problem
Traditional alert systems conflate Priority (clinical urgency) with Action Required (system needs input). This creates alert fatigue where clinicians dismiss critical warnings just to continue working, leading to preventable medical errors.
Intelligence Action Taxonomy Matrix
Decoupling Action from Urgency
HIGH PRIORITY
LOW PRIORITY
ACTION REQUIRED
NO ACTION REQUIRED
The Interpretation
Immediate threat. Requires human”Handshake”.
Reconcile to Chart
The State Awareness
Critical event. informs shared mental model.
Active Respiratory Distress
The FYI
Low-risk fields can be safely automated to reduce onboarding friction.
Pharmacy updated
The Housekeeping
System integrity task. Address during admin time.
Verify Patient Info
Timeline Visual System
Multimodal Encoding
Progressive disclosure through three-stage scaling and verification state encoding
Icons are hard to see in passive timeline views. This system maintains clarity without cluttering the screen through intelligent scale transitions and semantic color+glyph pairing.
Three-Stage Scaling Strategy
Progressive visual complexity based on user engagement level
16px
Stage 1: Passive
Small dot only. No icon. Keeps the "spine" clean for scrolling through long timelines. Low cognitive load.
32px on hover
Stage 2: Focus
On hover/scroll proximity, node expands to 16px and white glyph fades in. The "Aha!" moment where category is confirmed.
L1: Medication Order
L2: Verified by clinician
02/12 14:08
24px icon in card header
Stage 3: Object
Inside Intel Object Card, icon appears at 24px next to L1 Signal text. Full context revealed.
Why These Patterns
Tradeoffs Under Real-world Constraints
Patterns were selected to fit real systems, not idealized workflows
These patterns were chosen to:
- Respect existing systems of record
- Work across multiple environments
- Minimize workflow disruption
- Allow trust to build incrementally
Why not dashboards?
They centralize information but pull users out of real workflows.
Why not alerts everywhere?
They compete with native warnings and accelerate alert fatigue.
Why not overlays by default?
They interrupt primary tasks and don’t scale across systems.
Structural Evolution
From fragmented workspaces to AI-curated chronology
Anatomy of a Clinical Intelligence Object
A four-layer metadata hierarchy ensuring explainability through Signal,Insight, Rationale, and Evidence
Insight
L1
Semantic Interpretation
Semantic synthesis generated by TOON-AI. Natural language interpretation transforms raw clinical data into actionable intelligence.
TOON-AI Semantic Engine
Signal
L2
Ambient confidence
Confidence Score mapped to opacity pulse. Visual indicator provides immediate ambient awareness of data reliability without cognitive overhead.
JSON-AI Evidence Engine
Patient Alert
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Troponin I
0.8 ng/mL ↑
BNP
420 pg/mL ↑
HIGH 94% Confidence details
Pattern recognition: Troponin elevation (baseline 0.02→0.8) combined with BNP rise (180→420) over 6hrs. Correlates with EKG changes at 02:34. Rule: biomarker_velocity + temporal_clustering → alert_priority_high
Evidence Trail
Source Record
Lab_2026-02-12_0834
HIPAA Encrypted Deep-link
L3
Rationale
Reasoning Path
Hidden behind hover/dwell interaction to reduce visual noise. Reveals the computational logic and decision tree that led to this insight, maintaining transparency without overwhelming the interface
TOON-AI Semantic Engine
L4
Evidence
Source Attribution
Direct deep-link to source EHR record with HIPAA encryption. Enables immediate audit trail and source verification, critical for clinical decision support and regularity compliance.
JSON-AI Evidence Engine
JSON-AI (Evidence Engine)
TOON-AI (Semantic + Logic)
Core Flow Walkthrough
Interaction Map & Progressive Disclosure
Progressive disclosure: from ambient awareness to clinical decision
Two UI patterns: Continuity Strip (State 1-3) and Tieline Navigation (State 4)
State 1
Passive
The Glance
None
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
State 2
300ms Hover
The Lean-In (Dwell)
Hover
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
L3
Medication Discrepancy
Critical
Confidence: 94%
Metformin 1000mg BID found in CVS community record (filled 02/10), but missing from Epic chart. Patient reported taking medication during intake.
View Details
State 3
Click
The Audit (Action)
Click to expand
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
Medication Discrepancy Analysis
Evidence Deep-Dive
Source Comparison
Epic (Current)
No Metformin recorded
CVS Record
Metformin 1000mg BID
Filled: 02/10/2026
L4
Confidence: 94%
CVS_RX_2026-10_08:34:22
Prescription filled by Pharmacy ID: CVS-2847
Patient_Intake_2026-02-13_07:12:03
Verbal confirmation during admission
Epic_MedRec_Last_Updated_0225-11-03
Verbal confirmation during admission
Clinical Decision
Reconcile to Chart
Dismiss Alert
HIPAA Encrypted Deep-link
Continuity Strip: Progressive Disclosure
1
Passive Awareness
Ambient signals require zero cognitive load. Visual pulse communicates importance without interrupting workflows
2
contextual Insight
300ms dwell threshold reveals reasoning. Just-in-time information prevents alert fatigue while maintaining transparency
3
Verifiable Action
Full audit trail with clinical handshake. Every decision is traceable, reversible, and compliant with regulatory requirements
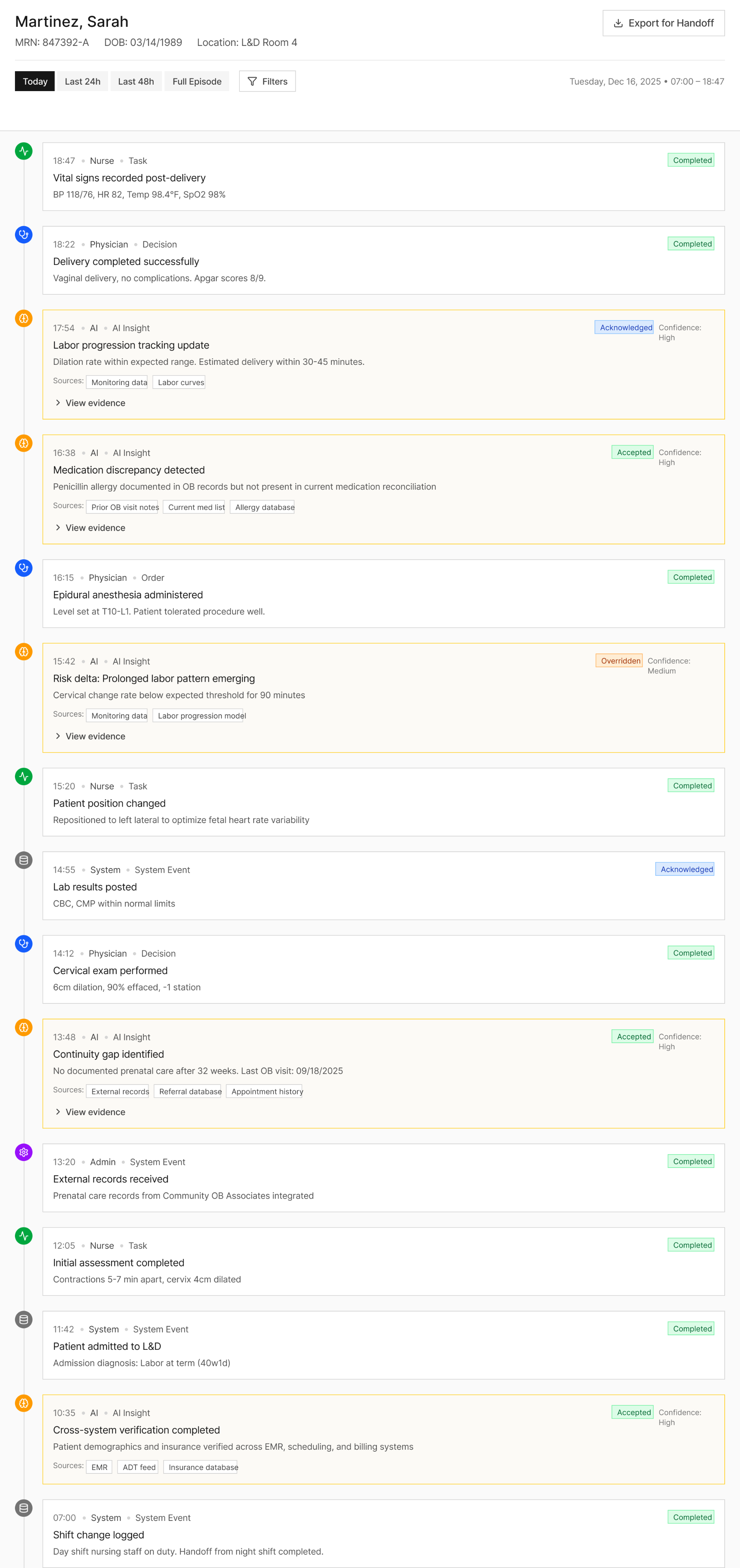
Shared Timeline
This isn’t a dashboard. It’s system memory
Why it exists
- Shift handoffs
- End-of-day review
- Cross-role reconciliation
What it shows
- Decisions and overrides
- AI insights with confidence
- Evidence trails across time
Systems Impact
Measuring Success
Validating continuity without increasing risk
What I’d Measure
Time to orientation
How quickly users understand what changed and what matters
Clarification loops
Back-and-forth caused by missing or unclear context
Scheduling failures
Downstream breakdowns caused by incomplete handoffs
AI insights acceptance vs override rates
A proxy for trust and signal quality
What I’d Test
- Confidence threshold tuning
- Role-based prioritization of insights
- Signal fatigue over time
Design Principle
AI earns trust by reducing work, not by demanding belief
Risks & Open Questions
Designing AI for real-world systems, not ideal conditions
Human Reality
- Trust must be earned
- Workflow disruption causes rejection
- Training and change fatigue are real
Integration Reality
- Varying EMR capabilities
- Limited control over host UI
- Long enterprise deployment cycles
Data Reality
- Incomplete records
- conflicting sources
- delayed or stale inputs
Design Responses & Mitigations
Core
Low Risk
Sidecar architeture
(low integration risk)
Alert
Info
Visual separation from system alerts
CTRL
Explicit human confirmation and override
Let’s Work Together
Interested in collaborating on complex UI/UX challenges involving data, AI, or enterprise systems?
I’d love to explore how thoughtful design can drive clarity and business impact.
Get In Touch
About Kelli
Product Designer | AI x Data Systems
Passionate about turning complex data and AI systems into clear, trustworthy, human-centered experiences
Based in: San Francisco, CA
© 2026 Kelli Nordfelt
Overview
Problem
Technical Wall
Design Pivot
System Impact
Retrospective
Overview
Designing AI Continuity in High Stakes Systems
Healthcare workflows break not because of a lack of data. They break because context doesn’t survive transitions.
Problem Framing
Stabilize Continuity • Predictive Reasoning • Not Automate Decisions
Why This Matters
Recent research highlights the importance of understanding patient state over time, not just at isolated moments.
MIRA: A Medical Foundation Model (NeurIPS)
Explores longitudinal modeling of medical data to enable more holistic insights across conditions.
This project applies that insight at the workflow level:
How continuity can be preserved across roles, systems, and handoffs without replacing human judgment.
The Hero Problem
Clinical continuity breaks across role boundaries and system transitions, forcing humans to rebuild context manually
High Cognitive Load • Repeated Work • Trust Gaps in AI tools
5 Day Product Design Sprint – From Discovery to Prototype
From scattered point points to a shared systemic problem
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
Problem Locked
Concept Selected
Prototype Ready
Objectives
Problem Framing
Analyze Current State
Ideate & Select
Build Prototype
Present & Plan
Research
& Discovery
Analyze current state
Synthesis
Current-State Mapping
Systems
& Design Thinking
Failure Analysis
AI Opportunity Framing
Prototyping
Low-fidelity flows
Core Flow Prototype
Persona Summaries
Final Narrative & Metrics
Deliverables
Workflow Diagram
Low-Fi Screens
Rapid Prototypes
The Problem & Discovery
Mapping the Shared Reality
From Retrieval to Proactive Delivery – The AI Layer
Identifying how Nurses, Physicians, and Specialists interact with data during crisis moments
Discovery & Interviews
Who I Spoke With
- Child & Adolescent Psychiatrist
- OB/GYN
- Maternal Fetal Medicine Physician (MFM)
- Registered Nurse (RN)
- Registration / Admin
What I Listened For
- Handoffs
- Cognitive load
- Risk points
- Trust boundaries
- AI adoption barriers
Physicians
“So many of our decisions are time-sensitive, but the information we need is often incomplete or scattered. I’m constantly double-checking because I don’t trust that I’m seeing the full picture.”
Breaks Today
Fragmented context, repeated documentation, low trust in prior data
Needs
Clear deltas, confidence-scored risks, evidence with human override
Nurses
“I’m interrupted constantly. I rely on quick signals to know what actually matters right now, but I still end up manually checking charts to make sure nothing critical was missed.”
Breaks Today
Interruptions, alert overload, manual safety checks
Needs
Prioritized tasks, trend signals, shift-safe handoffs
Admins
“When information is missing or changes without warning, we’re the ones trying to fix it. A small data issue upstream can turn into scheduling failures and patient frustration.”
Breaks Today
Missing context, silent automation failures, unclear urgency
Needs
Early risk signals, dependency visibility, auditable fixes
Emerging Themes & Cross-role Patterns
This validated continuity as a systemic problem, not UI issues
- Timing-sensitive decisions with incomplete data
- AI tools that help in isolation, but don’t connect the system
- Manual verification loops
- Repeated documentation
- Context loss at handoffs
Emerging Problem Themes Across the Clinical Continuity Ecosystem
Patterns observed across clinicians, operations, and frontline care during discovery interviews
High-risk convergence across roles
Localized role friction
Physicians
Nurses
Admins
Handoff & Shift Change Failures
- Critical clinical context lost during shift changes and cross-team transfers
- Time-sensitive risk factors not reliably surface to incoming physicians
- Incomplete handoffs from triage to registration
- Bed assignment confusion during shift change
- Med changes not communicated to oncoming staff
- Vital sign trends lost across shift boundaries
Medication List Accuracy
- Polypharmacy and cross-specialty interaction not visible at decision time
- Physicians manually double-check meds due to low system trust
- Patient self-reports unreliable or incomplete
- Insurance formulary gaps delay care start
- Reconciliation time burden delays admission
- Allergy documentation incomplete or outdated
Intake & Identity Validation
- External records and prior specialty care not consistently linked
- Emergency or consult scenarios bypass full intake validation
- Manual ID verification slows throughput
- Duplicate records created under time pressure
- Bedside ID checks and friction to workflow
- Patient wristband errors require rework
Scheduling & Throughput Breakdowns
- Consult timing and delivery decisions lack real-time clinical prioritization
- Delays in specialist coordination disrupt care continuity
- Check-in delays create bottlenecks at intake
- System downtime forces manual scheduling workarounds
- Discharge delays block incoming patient flow
- Float staff lack unit-specific context
Documentation Overload
- High-risk cases require extensive documentation beyond available time
- Repetitive note-writing replaces clinical reasoning and patient interaction
- Redundant data entry across intake workflows
- Scanning backlog delays chart availability
- Charting burden limits bedside presence
- Alert fatigue from documentation promopts
Trust in Systems
- Alert fatigue leads to ignored or overridden system warnings
- Decision supprt lacks transparency for edge-case clinical judgment
- System outages force paper fallback distrust
- data accuracy concerns affect downstream care
- Alert overrides become routine due to volume
- System lag undermines real-time decision-making
AI Adoption Barriers
- Liability concerns around AI-assisted recommendations
- Limited training on interpreting AI confidence and uncertainty
- Fear of role displacement by automation
- Lack of agency in AI implementation decisions
- Workflow disruption concerns outweigh benefits
- Training gaps for AI-enhanced clinical tools
What Must Stay Human
- Complex risk-benefit decisions made collaboratively with patients
- Ethical accountability in high-stakes clinical outcomes
- Empathy during high-stress registration moments
- Cultural navigation and language access
- Patient comfort and bedside presence
- Advocacy and care coordination across teams
The Technical Wall
From Retrieval to Proactive Context
Why clinicians are forced to rebuild context by hand
Current-State Clinical Workflow: Fragmented Continuity of Care
Where Fragmentation, Repetition, and Trust Gaps Occur
Human Input
Decision Moment
Operational Systems
External Sources
EHR System (CoreHealth)
Info Artifact
View Failure Points

Provider
Examination
Imaging Orders
Lab Orders
Clinical Decision Moment


Triage & Assessment

Results Review
& Analysis




Insurance Verification




EHR System
(CoreHealth)




Lab system
(LabCore)

Outside
Hospital Records

Patient Interview
(Verbal)

Patient Arrives

Patient Mobile
Check-In App
Front Desk Registration

Scheduling System

Billing System
(PaymentMate)
Department Coordination

Specialty
Consultation
Patient
Discharge
Discharge Instructions
Imaging System
(RadView)

Shift-Change
Handoff (Verbal)

Medication
Reconciliation















7
Human Touchpoint’s
(Many-to-Many Communication Load)
4
External Data Sources
(Many-to-Many Fragmentation Risk)
4
High-Stakes
Decision Moments
1
Central EHR Record
(Single Source of Truth, Limited Context)
7
Operational Systems per Patient Journey
(1-to-Many Integration Burden)
Fragmented Inputs Create Hidden Clinical Risk
Care teams must coordinate across multiple human handoffs, disconnected operational systems, and incomplete external records. The EHR acts as a central hub, but critical context remains distributed, forcing clinicians to bridge gaps manually during high-stakes decision moments.
AI Opportunity Framework
Two complementary AI Layers Working Together
JSON-AI Layer
(Structured Intelligence)
Structured continuity intelligence
- Medication reconciliation
- Scheduling logic & insurance verification
- Clean summaries
- Continuity “checklist” generation
TOON-AI Layer
(Narrative/Reasoning AI)
Interpretive reasoning
- Nuance-finding in handoffs
- Rick deltas
- Inconsistencies in the patient story
- Reasoning across notes and conversations
- Role-specific briefings
AI restores context so human judgment can be used with confidence
Future-State: AI Continuity Platform Across the Care Journey
A clean, technical systems diagram showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
AI Continuity Platform
A clean, technical systems showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
Patient
Identity Resolution
JSON AI
Cross-System Data Normalization
JSON AI
Predictive Risk
& Timing Engine
ML/LLM
Continuity
Thread Tracker
TOON AI
Clinical
Decision Assist
LLM
Smart Documentation
& Summaries
LLM
Task Routing & Workflow Automation
JSON AI
Care Team
Communication Layer
JSON AI
Registration / Admin
Intake Capture
Eligibility & Verification
Automated Follow-up Tasks
Documentation Prep
Nurse
Pre-visit Checklist
Care Gaps Identified
Alerts & Risk Signals
Cross-Encounter Summaries
Primary OB / Specialist
Longitudinal Pregnancy Timeline
Ultrasound & Labs Auto-Summary
Treatment Path Proposals
Moment-to-Moment Risk Predictions
Psychiatry Behavioral
Medication Interactions Highlights
Behavioral Risk Predictions
Aggregated narrative Summaries
Patient
Intelligent Appointment Prep
Tailored Education
Self-Reported Outcomes
Cross-Visit Care Plan View
Continuity Thread maintains narrative across encounters
JSON AI resolves structured discrepancies
TOON AI reconstructs tacit, human-contextual meaning
LLM suggests next actions but requires clinician oversight
Underlying Systems (Future Harmonized AI)
EHR (Epic/Cerner etc.)
structured → JSON AI
Labs and Imaging systems
structured → JSON AI
Pharmacy Systems
structured → JSON AI
Scheduling Systems
structured → JSON AI
Billing / Claims / Eligibility
structured → JSON AI
External Data
(Wearables, HIE)
Multi-mode → TOON






8
AI Platform Modules
5
Persona Workflows
6
Integrated Systems
19
Failures Resolved
100%
Continuity Coverage
Design Pivot
Designing the Clinical Intelligence Layer
Different surfaces. Same continuity intelligence
Continuity cannot live in a single interface. It must persist across roles, tools, and time
Three Patterns for AI-Supported Continuity
To avoid “Dashboard Fatigue,” we can move explainability to the object level. Each insight adapts to the persona while utilizing three core patterns.
Continuity Strip
- Explainable, cross-system, non-blocking
- Persistent continuity without competing with system alerts
Sidecar Panel
- System memory across roles and time
- Handoffs, overrides, and reasoning in one place
Shared Timeline
- Moment-of-decision context
- What changed, what matters now, What is next
Persona-Specific Workflows
AI utility is not one-size-fits-all
The system surfaces the same “Intelligence Object” in different formats depending on the user’s role” Physicians receive deep-dive rationale for diagnosis, Nurses see actionable safety threads during handoff, and Admins receive operational status updates to clear discharge bottlenecks.
One Critical Event, Three Interpretations
An external record from St. Mary’s Hospital arrives at 08:42 AM, revealing HIGH-RISK PENICILLIN ALLERGY not documented in the Epic chart. The AI detects this discrepancy and surfaces it differently for each decision owner’s specific pressure points.
Dr. Aris Chen
Attending Physician
Primary Goal
Validate diagnostic risk & maintain accuracy
Decision Pressure Points:
- Deep work mode, cannot tolerate interruptions
- Needs full evidence trail for liability
- Must understand "why" before acting
UI Pattern: The Sidecar Panel
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
AI Continuity
Context for this shift
Patient Insights
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Evidence Trail
St. Mary’s discharge summary (02/10) • Confirmed via FHIR import • Verified anaphylaxis history
The Clinical Handshake:
Verify & Update Chart
Flag as Error
Human remains final authority. Action logged to audit trail.
Sarah Martinez, RN
Charge Nurse
Primary Goal
Execute safe tasks during handoff
Decision Pressure Points:
- High task density—needs glanceable safety checks
- Shift handoff = critical error window
- Must act fast without missing context
UI Pattern: The Shared Timeline
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Medication Administration
Scheduled Administration
10:00
Amoxicillin 500mg PO
ALLERGY CONFLICT
Critical
Penicillin allergy detected in external record. Amoxicillin is contraindicated.
HIGH
94% Confidence
Auto-flagged
Scheduled assessment
14:00
Amoxicillin 500mg PO
The Clinical Handshake:
Hold Medication
Page Provider
Error prevented. Intervention escalated to physician.
Marcus Kim
Care Coordinator
Primary Goal
Clear discharge bottlenecks & ensure compliance
Decision Pressure Points:
- Manages 40+ patients and needs status at-a-glance
- Doesn’t need clinical PII< just completion status
- Discharge delays = throughput bottlenecks
UI Pattern: Exception-Based Alert Feed
No dashboard to monitor. System PUSHES critical blockers to the feed. Silent when everything flows smoothly.
Active Discharge Blocker Detected
Patient 847-2931
Ready
Patient 847-2931
✓ Now Complete
Status Update
Critical data gap resolved at 08:47
Allergy record reconciled & verified
Patient 847-2931
Pending...
The Clinical Handshake:
Mark Discharge-Ready
View Full Feed
Bottleneck cleared. Patient ready for discharge workflow.
The Clinical Handshake: Closing the Loop
Regardless of role, every interaction ends in a HANDSHAKE. A deliberate human action that confirms or rejects the AI’s synthesis. This ensures that while the AI handles the data plumbing, the human remains the final authority in the clinical record.
Physician
Verify & update with full audit trail
Nurse
Hold medication & escalate to provider
Admin
Mark complete & clear bottleneck
Structural Evolution
From fragmented workspaces to AI-curated chronology
Before
Fragmented Workspaces
TAB CHAOS
Patient
Labs
Med Rec
+8
Verbal Note (Tab 1)
“Patient reports taking Metformin...”
Nurse intake 02/13
Outside PDF (Tab 3)
St. Mary's Hospital Discharge Summary
Scanned: 01/10/2026
Lab Result (Tab 2)
Troponin: 0.8 ng/mL
01/12/2026 13:34
Med Rec (Tab 4)
“Patient reports taking Metformin...”
103 days old

Manual
Integration
After
AI-Curated Timeline
UNIFIED CHRONOLOGY
Shared Timeline
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Outside Hospital Discharge
02/10/ 14:22
St. Mary’s Hospital • Cardiac Event
JSON-AI auto-parsed PDF
Matched: Discharge RX → Pharmacy
Pharmacy Fill
Metformin 1000mg BID • CVS Pharmacy
TOON-AI linked to discharge orders
02/10/ 16:45
Verified: Nurse note ↔ Pharmacy
Lab Result Anomaly
Troponin I: 0.8 ng/mL ↑ (Critical)
JSON-AI flagged spike pattern
02/12/ 08:34
Linked: Cardiac event → Lab spike
Intake Verification
Nurse confirmed Metformin use verbally
TOON-AI reconciled with CVS record
02/13/ 07:12
Matched: Discharge RX → Parmacy
AI-Insight
Med discrepancy + cardiac markers = High-risk patterns
Now
HIGH
94% Confidence
Auto-flagged before first dose
The Clinical Handshake: Closing the Loop
Problem
Data fragmentation forces clinicians to become “human middleware,” manually integrating disparate sources.
Solution
AI becomes the integration layer, automatically reconciling cross-system data into a unified temporal model.
Impact
Clinicians focus on care decisions, not data archeaology. Critical patterns emerge from temporal synthesis
Action vs. Priority
Preventing Compliance Fatigue
In high-stakes systems, you must distinguish between Actionable Intelligence and Critical Awareness
If you force an "Action" on everything that is "High Priority," you create a "Compliance UI" where users click "OK" just to clear the screen—which is how major medical errors happen.
The Compliance Fatigue Problem
Traditional alert systems conflate Priority (clinical urgency) with Action Required (system needs input). This creates alert fatigue where clinicians dismiss critical warnings just to continue working, leading to preventable medical errors.
Intelligence Action Taxonomy Matrix
Decoupling Action from Urgency
HIGH PRIORITY
LOW PRIORITY
ACTION REQUIRED
NO ACTION REQUIRED
The Interpretation
Immediate threat. Requires human”Handshake”.
Reconcile to Chart
The State Awareness
Critical event. informs shared mental model.
Active Respiratory Distress
The FYI
Low-risk fields can be safely automated to reduce onboarding friction.
Pharmacy updated
The Housekeeping
System integrity task. Address during admin time.
Verify Patient Info
Timeline Visual System
Multimodal Encoding
Progressive disclosure through three-stage scaling and verification state encoding
Icons are hard to see in passive timeline views. This system maintains clarity without cluttering the screen through intelligent scale transitions and semantic color+glyph pairing.
Three-Stage Scaling Strategy
Progressive visual complexity based on user engagement level
16px
Stage 1: Passive
Small dot only. No icon. Keeps the "spine" clean for scrolling through long timelines. Low cognitive load.
32px on hover
Stage 2: Focus
On hover/scroll proximity, node expands to 16px and white glyph fades in. The "Aha!" moment where category is confirmed.
L1: Medication Order
L2: Verified by clinician
02/12 14:08
24px icon in card header
Stage 3: Object
Inside Intel Object Card, icon appears at 24px next to L1 Signal text. Full context revealed.
Why These Patterns
Tradeoffs Under Real-world Constraints
Patterns were selected to fit real systems, not idealized workflows
These patterns were chosen to:
- Respect existing systems of record
- Work across multiple environments
- Minimize workflow disruption
- Allow trust to build incrementally
Why not dashboards?
They centralize information but pull users out of real workflows.
Why not alerts everywhere?
They compete with native warnings and accelerate alert fatigue.
Why not overlays by default?
They interrupt primary tasks and don’t scale across systems.
Structural Evolution
From fragmented workspaces to AI-curated chronology
Anatomy of a Clinical Intelligence Object
A four-layer metadata hierarchy ensuring explainability through Signal,Insight, Rationale, and Evidence
Insight
L1
Semantic Interpretation
Semantic synthesis generated by TOON-AI. Natural language interpretation transforms raw clinical data into actionable intelligence.
TOON-AI Semantic Engine
Signal
L2
Ambient confidence
Confidence Score mapped to opacity pulse. Visual indicator provides immediate ambient awareness of data reliability without cognitive overhead.
JSON-AI Evidence Engine
Patient Alert
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Troponin I
0.8 ng/mL ↑
BNP
420 pg/mL ↑
HIGH 94% Confidence details
Pattern recognition: Troponin elevation (baseline 0.02→0.8) combined with BNP rise (180→420) over 6hrs. Correlates with EKG changes at 02:34. Rule: biomarker_velocity + temporal_clustering → alert_priority_high
Evidence Trail
Source Record
Lab_2026-02-12_0834
HIPAA Encrypted Deep-link
L3
Rationale
Reasoning Path
Hidden behind hover/dwell interaction to reduce visual noise. Reveals the computational logic and decision tree that led to this insight, maintaining transparency without overwhelming the interface
TOON-AI Semantic Engine
L4
Evidence
Source Attribution
Direct deep-link to source EHR record with HIPAA encryption. Enables immediate audit trail and source verification, critical for clinical decision support and regularity compliance.
JSON-AI Evidence Engine
JSON-AI (Evidence Engine)
TOON-AI (Semantic + Logic)
Core Flow Walkthrough
Interaction Map & Progressive Disclosure
Progressive disclosure: from ambient awareness to clinical decision
Two UI patterns: Continuity Strip (State 1-3) and Tieline Navigation (State 4)
State 1
Passive
The Glance
None
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
State 2
300ms Hover
The Lean-In (Dwell)
Hover
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
L3
Medication Discrepancy
Critical
Confidence: 94%
Metformin 1000mg BID found in CVS community record (filled 02/10), but missing from Epic chart. Patient reported taking medication during intake.
View Details
State 3
Click
The Audit (Action)
Click to expand
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
Medication Discrepancy Analysis
Evidence Deep-Dive
Source Comparison
Epic (Current)
No Metformin recorded
CVS Record
Metformin 1000mg BID
Filled: 02/10/2026
L4
Confidence: 94%
CVS_RX_2026-10_08:34:22
Prescription filled by Pharmacy ID: CVS-2847
Patient_Intake_2026-02-13_07:12:03
Verbal confirmation during admission
Epic_MedRec_Last_Updated_0225-11-03
Verbal confirmation during admission
Clinical Decision
Reconcile to Chart
Dismiss Alert
HIPAA Encrypted Deep-link
Continuity Strip: Progressive Disclosure
1
Passive Awareness
Ambient signals require zero cognitive load. Visual pulse communicates importance without interrupting workflows
2
contextual Insight
300ms dwell threshold reveals reasoning. Just-in-time information prevents alert fatigue while maintaining transparency
3
Verifiable Action
Full audit trail with clinical handshake. Every decision is traceable, reversible, and compliant with regulatory requirements
Shared Timeline
This isn’t a dashboard. It’s system memory
Why it exists
- Shift handoffs
- End-of-day review
- Cross-role reconciliation
What it shows
- Decisions and overrides
- AI insights with confidence
- Evidence trails across time
Systems Impact
Measuring Success
Validating continuity without increasing risk
What I’d Measure
Time to orientation
How quickly users understand what changed and what matters
Clarification loops
Back-and-forth caused by missing or unclear context
Scheduling failures
Downstream breakdowns caused by incomplete handoffs
AI insights acceptance vs override rates
A proxy for trust and signal quality
What I’d Test
- Confidence threshold tuning
- Role-based prioritization of insights
- Signal fatigue over time
Design Principle
AI earns trust by reducing work, not by demanding belief
Risks & Open Questions
Designing AI for real-world systems, not ideal conditions
Human Reality
- Trust must be earned
- Workflow disruption causes rejection
- Training and change fatigue are real
Integration Reality
- Varying EMR capabilities
- Limited control over host UI
- Long enterprise deployment cycles
Data Reality
- Incomplete records
- conflicting sources
- delayed or stale inputs
Design Responses & Mitigations
Core
Low Risk
Sidecar architeture
(low integration risk)
Alert
Info
Visual separation from system alerts
CTRL
Explicit human confirmation and override
Let’s Work Together
Interested in collaborating on complex UI/UX challenges involving data, AI, or enterprise systems?
I’d love to explore how thoughtful design can drive clarity and business impact.
Get In Touch
About Kelli
Product Designer | AI x Data Systems
Passionate about turning complex data and AI systems into clear, trustworthy, human-centered experiences
Based in: San Francisco, CA
© 2026 Kelli Nordfelt
Overview
Problem
Technical Wall
Design Pivot
System Impact
Retrospective


Overview

Problem

Technical Wall

Design Pivot

System Impact

Retrospective
Overview
Designing AI Continuity in High Stakes Systems
Healthcare workflows break not because of a lack of data. They break because context doesn’t survive transitions.
Problem Framing
Stabilize Continuity • Predictive Reasoning • Not Automate Decisions
Why This Matters
Recent research highlights the importance of understanding patient state over time, not just at isolated moments.
MIRA: A Medical Foundation Model (NeurIPS)
Explores longitudinal modeling of medical data to enable more holistic insights across conditions.
This project applies that insight at the workflow level:
How continuity can be preserved across roles, systems, and handoffs without replacing human judgment.
The Hero Problem
Clinical continuity breaks across role boundaries and system transitions, forcing humans to rebuild context manually
High Cognitive Load • Repeated Work • Trust Gaps in AI tools
5 Day Product Design Sprint – From Discovery to Prototype
From scattered point points to a shared systemic problem
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
Problem Locked
Concept Selected
Prototype Ready
Objectives
Problem Framing
Analyze Current State
Ideate & Select
Build Prototype
Present & Plan
Research
& Discovery
Analyze current state
Synthesis
Current-State Mapping
Systems
& Design Thinking
Failure Analysis
AI Opportunity Framing
Prototyping
Low-fidelity flows
Core Flow Prototype
Persona Summaries
Final Narrative & Metrics
Deliverables
Workflow Diagram
Low-Fi Screens
Rapid Prototypes
The Problem & Discovery
Mapping the Shared Reality
From Retrieval to Proactive Delivery – The AI Layer
Identifying how Nurses, Physicians, and Specialists interact with data during crisis moments
Discovery & Interviews
Who I Spoke With
- Child & Adolescent Psychiatrist
- OB/GYN
- Maternal Fetal Medicine Physician (MFM)
- Registered Nurse (RN)
- Registration / Admin
What I Listened For
- Handoffs
- Cognitive load
- Risk points
- Trust boundaries
- AI adoption barriers
Physicians
“So many of our decisions are time-sensitive, but the information we need is often incomplete or scattered. I’m constantly double-checking because I don’t trust that I’m seeing the full picture.”
Breaks Today
Fragmented context, repeated documentation, low trust in prior data
Needs
Clear deltas, confidence-scored risks, evidence with human override
Nurses
“I’m interrupted constantly. I rely on quick signals to know what actually matters right now, but I still end up manually checking charts to make sure nothing critical was missed.”
Breaks Today
Interruptions, alert overload, manual safety checks
Needs
Prioritized tasks, trend signals, shift-safe handoffs
Admins
“When information is missing or changes without warning, we’re the ones trying to fix it. A small data issue upstream can turn into scheduling failures and patient frustration.”
Breaks Today
Missing context, silent automation failures, unclear urgency
Needs
Early risk signals, dependency visibility, auditable fixes
Emerging Themes & Cross-role Patterns
This validated continuity as a systemic problem, not UI issues
- Timing-sensitive decisions with incomplete data
- AI tools that help in isolation, but don’t connect the system
- Manual verification loops
- Repeated documentation
- Context loss at handoffs
Emerging Problem Themes Across the Clinical Continuity Ecosystem
Patterns observed across clinicians, operations, and frontline care during discovery interviews
High-risk convergence across roles
Localized role friction
Physicians
Nurses
Admins
Handoff & Shift Change Failures
- Critical clinical context lost during shift changes and cross-team transfers
- Time-sensitive risk factors not reliably surface to incoming physicians
- Incomplete handoffs from triage to registration
- Bed assignment confusion during shift change
- Med changes not communicated to oncoming staff
- Vital sign trends lost across shift boundaries
Medication List Accuracy
- Polypharmacy and cross-specialty interaction not visible at decision time
- Physicians manually double-check meds due to low system trust
- Patient self-reports unreliable or incomplete
- Insurance formulary gaps delay care start
- Reconciliation time burden delays admission
- Allergy documentation incomplete or outdated
Intake & Identity Validation
- External records and prior specialty care not consistently linked
- Emergency or consult scenarios bypass full intake validation
- Manual ID verification slows throughput
- Duplicate records created under time pressure
- Bedside ID checks and friction to workflow
- Patient wristband errors require rework
Scheduling & Throughput Breakdowns
- Consult timing and delivery decisions lack real-time clinical prioritization
- Delays in specialist coordination disrupt care continuity
- Check-in delays create bottlenecks at intake
- System downtime forces manual scheduling workarounds
- Discharge delays block incoming patient flow
- Float staff lack unit-specific context
Documentation Overload
- High-risk cases require extensive documentation beyond available time
- Repetitive note-writing replaces clinical reasoning and patient interaction
- Redundant data entry across intake workflows
- Scanning backlog delays chart availability
- Charting burden limits bedside presence
- Alert fatigue from documentation promopts
Trust in Systems
- Alert fatigue leads to ignored or overridden system warnings
- Decision supprt lacks transparency for edge-case clinical judgment
- System outages force paper fallback distrust
- data accuracy concerns affect downstream care
- Alert overrides become routine due to volume
- System lag undermines real-time decision-making
AI Adoption Barriers
- Liability concerns around AI-assisted recommendations
- Limited training on interpreting AI confidence and uncertainty
- Fear of role displacement by automation
- Lack of agency in AI implementation decisions
- Workflow disruption concerns outweigh benefits
- Training gaps for AI-enhanced clinical tools
What Must Stay Human
- Complex risk-benefit decisions made collaboratively with patients
- Ethical accountability in high-stakes clinical outcomes
- Empathy during high-stress registration moments
- Cultural navigation and language access
- Patient comfort and bedside presence
- Advocacy and care coordination across teams
The Technical Wall
From Retrieval to Proactive Context
Why clinicians are forced to rebuild context by hand
Current-State Clinical Workflow: Fragmented Continuity of Care
Where Fragmentation, Repetition, and Trust Gaps Occur
Human Input
Decision Moment
Operational Systems
External Sources
EHR System (CoreHealth)
Info Artifact
View Failure Points
Provider
Examination
Imaging Orders
Lab Orders
Clinical Decision Moment
Triage & Assessment
Results Review
& Analysis
Insurance Verification
EHR System
(CoreHealth)
Lab system
(LabCore)
Outside
Hospital Records
Patient Interview
(Verbal)
Patient Arrives
Patient Mobile
Check-In App
Front Desk Registration
Scheduling System
Billing System
(PaymentMate)
Department Coordination
Specialty
Consultation
Patient
Discharge
Discharge Instructions
Imaging System
(RadView)
Shift-Change
Handoff (Verbal)
Medication
Reconciliation
7
Human Touchpoint’s
(Many-to-Many Communication Load)
4
External Data Sources
(Many-to-Many Fragmentation Risk)
4
High-Stakes
Decision Moments
1
Central EHR Record
(Single Source of Truth, Limited Context)
7
Operational Systems per Patient Journey
(1-to-Many Integration Burden)
Fragmented Inputs Create Hidden Clinical Risk
Care teams must coordinate across multiple human handoffs, disconnected operational systems, and incomplete external records. The EHR acts as a central hub, but critical context remains distributed, forcing clinicians to bridge gaps manually during high-stakes decision moments.
AI Opportunity Framework
Two complementary AI Layers Working Together
JSON-AI Layer
(Structured Intelligence)
Structured continuity intelligence
- Medication reconciliation
- Scheduling logic & insurance verification
- Clean summaries
- Continuity “checklist” generation
TOON-AI Layer
(Narrative/Reasoning AI)
Interpretive reasoning
- Nuance-finding in handoffs
- Rick deltas
- Inconsistencies in the patient story
- Reasoning across notes and conversations
- Role-specific briefings
AI restores context so human judgment can be used with confidence
Future-State: AI Continuity Platform Across the Care Journey
A clean, technical systems diagram showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
AI Continuity Platform
A clean, technical systems showing how an AI Continuity Platform unifies today's fragmented healthcare workflows into a seamless, intelligent care journey.
Patient
Identity Resolution
JSON AI
Cross-System Data Normalization
JSON AI
Predictive Risk
& Timing Engine
ML/LLM
Continuity
Thread Tracker
TOON AI
Clinical
Decision Assist
LLM
Smart Documentation
& Summaries
LLM
Task Routing & Workflow Automation
JSON AI
Care Team
Communication Layer
JSON AI
Registration / Admin
Intake Capture
Eligibility & Verification
Automated Follow-up Tasks
Documentation Prep
Nurse
Pre-visit Checklist
Care Gaps Identified
Alerts & Risk Signals
Cross-Encounter Summaries
Primary OB / Specialist
Longitudinal Pregnancy Timeline
Ultrasound & Labs Auto-Summary
Treatment Path Proposals
Moment-to-Moment Risk Predictions
Psychiatry Behavioral
Medication Interactions Highlights
Behavioral Risk Predictions
Aggregated narrative Summaries
Patient
Intelligent Appointment Prep
Tailored Education
Self-Reported Outcomes
Cross-Visit Care Plan View
Continuity Thread maintains narrative across encounters
JSON AI resolves structured discrepancies
TOON AI reconstructs tacit, human-contextual meaning
LLM suggests next actions but requires clinician oversight
Underlying Systems (Future Harmonized AI)
EHR (Epic/Cerner etc.)
structured → JSON AI
Labs and Imaging systems
structured → JSON AI
Pharmacy Systems
structured → JSON AI
Scheduling Systems
structured → JSON AI
Billing / Claims / Eligibility
structured → JSON AI
External Data
(Wearables, HIE)
Multi-mode → TOON
8
AI Platform Modules
5
Persona Workflows
6
Integrated Systems
19
Failures Resolved
100%
Continuity Coverage
Design Pivot
Designing the Clinical Intelligence Layer
Different surfaces. Same continuity intelligence
Continuity cannot live in a single interface. It must persist across roles, tools, and time
Three Patterns for AI-Supported Continuity
To avoid “Dashboard Fatigue,” we can move explainability to the object level. Each insight adapts to the persona while utilizing three core patterns.
Continuity Strip
- Explainable, cross-system, non-blocking
- Persistent continuity without competing with system alerts
Sidecar Panel
- System memory across roles and time
- Handoffs, overrides, and reasoning in one place
Shared Timeline
- Moment-of-decision context
- What changed, what matters now, What is next
Persona-Specific Workflows
AI utility is not one-size-fits-all
The system surfaces the same “Intelligence Object” in different formats depending on the user’s role” Physicians receive deep-dive rationale for diagnosis, Nurses see actionable safety threads during handoff, and Admins receive operational status updates to clear discharge bottlenecks.
One Critical Event, Three Interpretations
An external record from St. Mary’s Hospital arrives at 08:42 AM, revealing HIGH-RISK PENICILLIN ALLERGY not documented in the Epic chart. The AI detects this discrepancy and surfaces it differently for each decision owner’s specific pressure points.
Dr. Aris Chen
Attending Physician
Primary Goal
Validate diagnostic risk & maintain accuracy
Decision Pressure Points:
- Deep work mode, cannot tolerate interruptions
- Needs full evidence trail for liability
- Must understand "why" before acting
UI Pattern: The Sidecar Panel
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
AI Continuity
Context for this shift
Patient Insights
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Evidence Trail
St. Mary’s discharge summary (02/10) • Confirmed via FHIR import • Verified anaphylaxis history
The Clinical Handshake:
Verify & Update Chart
Flag as Error
Human remains final authority. Action logged to audit trail.
Sarah Martinez, RN
Charge Nurse
Primary Goal
Execute safe tasks during handoff
Decision Pressure Points:
- High task density—needs glanceable safety checks
- Shift handoff = critical error window
- Must act fast without missing context
UI Pattern: The Shared Timeline
Non-intrusive signal on Continuity Strip. On "lean-in," full evidence panel slides out with rationale.
Medication Administration

Scheduled Administration
10:00
Amoxicillin 500mg PO
ALLERGY CONFLICT
Critical
Penicillin allergy detected in external record. Amoxicillin is contraindicated.
HIGH
94% Confidence
Auto-flagged

Scheduled assessment
14:00
Amoxicillin 500mg PO
The Clinical Handshake:
Hold Medication
Page Provider
Error prevented. Intervention escalated to physician.
Marcus Kim
Care Coordinator
Primary Goal
Clear discharge bottlenecks & ensure compliance
Decision Pressure Points:
- Manages 40+ patients and needs status at-a-glance
- Doesn’t need clinical PII< just completion status
- Discharge delays = throughput bottlenecks
UI Pattern: Exception-Based Alert Feed
No dashboard to monitor. System PUSHES critical blockers to the feed. Silent when everything flows smoothly.
Active Discharge Blocker Detected
Patient 847-2931
Ready
Patient 847-2931
✓ Now Complete
Status Update
Critical data gap resolved at 08:47
Allergy record reconciled & verified
Patient 847-2931
Pending...
The Clinical Handshake:
Mark Discharge-Ready
View Full Feed
Bottleneck cleared. Patient ready for discharge workflow.
The Clinical Handshake: Closing the Loop
Regardless of role, every interaction ends in a HANDSHAKE. A deliberate human action that confirms or rejects the AI’s synthesis. This ensures that while the AI handles the data plumbing, the human remains the final authority in the clinical record.
Physician
Verify & update with full audit trail
Nurse
Hold medication & escalate to provider
Admin
Mark complete & clear bottleneck
Structural Evolution
From fragmented workspaces to AI-curated chronology
Before
Fragmented Workspaces
TAB CHAOS
Patient
Labs
Med Rec
+8
Verbal Note (Tab 1)
“Patient reports taking Metformin...”
Nurse intake 02/13
Outside PDF (Tab 3)
St. Mary's Hospital Discharge Summary
Scanned: 01/10/2026
Lab Result (Tab 2)
Troponin: 0.8 ng/mL
01/12/2026 13:34
Med Rec (Tab 4)
“Patient reports taking Metformin...”
103 days old

Manual
Integration
After
AI-Curated Timeline
UNIFIED CHRONOLOGY
Shared Timeline
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Outside Hospital Discharge
02/10/ 14:22
St. Mary’s Hospital • Cardiac Event
JSON-AI auto-parsed PDF
Matched: Discharge RX → Pharmacy
Pharmacy Fill
Metformin 1000mg BID • CVS Pharmacy
TOON-AI linked to discharge orders
02/10/ 16:45
Verified: Nurse note ↔ Pharmacy
Lab Result Anomaly
Troponin I: 0.8 ng/mL ↑ (Critical)
JSON-AI flagged spike pattern
02/12/ 08:34
Linked: Cardiac event → Lab spike
Intake Verification
Nurse confirmed Metformin use verbally
TOON-AI reconciled with CVS record
02/13/ 07:12
Matched: Discharge RX → Parmacy
AI-Insight
Med discrepancy + cardiac markers = High-risk patterns
Now
HIGH
94% Confidence
Auto-flagged before first dose
The Clinical Handshake: Closing the Loop
Problem
Data fragmentation forces clinicians to become “human middleware,” manually integrating disparate sources.
Solution
AI becomes the integration layer, automatically reconciling cross-system data into a unified temporal model.
Impact
Clinicians focus on care decisions, not data archaeology. Critical patterns emerge from temporal synthesis
Action vs. Priority
Preventing Compliance Fatigue
In high-stakes systems, you must distinguish between Actionable Intelligence and Critical Awareness
If you force an "Action" on everything that is "High Priority," you create a "Compliance UI" where users click "OK" just to clear the screen—which is how major medical errors happen.
The Compliance Fatigue Problem
Traditional alert systems conflate Priority (clinical urgency) with Action Required (system needs input). This creates alert fatigue where clinicians dismiss critical warnings just to continue working, leading to preventable medical errors.
Intelligence Action Taxonomy Matrix
Decoupling Action from Urgency
HIGH PRIORITY
LOW PRIORITY
ACTION REQUIRED
NO ACTION REQUIRED
The Interpretation
Immediate threat. Requires human”Handshake”.
Reconcile to Chart
The State Awareness
Critical event. informs shared mental model.
Active Respiratory Distress
The FYI
Low-risk fields can be safely automated to reduce onboarding friction.
Pharmacy updated
The Housekeeping
System integrity task. Address during admin time.
Verify Patient Info
Timeline Visual System
Multimodal Encoding
Progressive disclosure through three-stage scaling and verification state encoding
Icons are hard to see in passive timeline views. This system maintains clarity without cluttering the screen through intelligent scale transitions and semantic color+glyph pairing.
Three-Stage Scaling Strategy
Progressive visual complexity based on user engagement level

16px
Stage 1: Passive
Small dot only. No icon. Keeps the "spine" clean for scrolling through long timelines. Low cognitive load.

32px on hover
Stage 2: Focus
On hover/scroll proximity, node expands to 16px and white glyph fades in. The "Aha!" moment where category is confirmed.
L1: Medication Order
L2: Verified by clinician
02/12 14:08
24px icon in card header
Stage 3: Object
Inside Intel Object Card, icon appears at 24px next to L1 Signal text. Full context revealed.
Why These Patterns
Tradeoffs Under Real-world Constraints
Patterns were selected to fit real systems, not idealized workflows
These patterns were chosen to:
- Respect existing systems of record
- Work across multiple environments
- Minimize workflow disruption
- Allow trust to build incrementally
Why not dashboards?
They centralize information but pull users out of real workflows.
Why not alerts everywhere?
They compete with native warnings and accelerate alert fatigue.
Why not overlays by default?
They interrupt primary tasks and don’t scale across systems.
Structural Evolution
From fragmented workspaces to AI-curated chronology
Anatomy of a Clinical Intelligence Object
A four-layer metadata hierarchy ensuring explainability through Signal,Insight, Rationale, and Evidence
Insight
L1
Semantic Interpretation
Semantic synthesis generated by TOON-AI. Natural language interpretation transforms raw clinical data into actionable intelligence.
TOON-AI Semantic Engine
Signal
L2
Ambient confidence
Confidence Score mapped to opacity pulse. Visual indicator provides immediate ambient awareness of data reliability without cognitive overhead.
JSON-AI Evidence Engine
Patient Alert
Critical
Elevated cardiac markers detected with trending deterioration over 6-hour window
Troponin I
0.8 ng/mL ↑
BNP
420 pg/mL ↑
HIGH 94% Confidence details
Pattern recognition: Troponin elevation (baseline 0.02→0.8) combined with BNP rise (180→420) over 6hrs. Correlates with EKG changes at 02:34. Rule: biomarker_velocity + temporal_clustering → alert_priority_high
Evidence Trail
Source Record
Lab_2026-02-12_0834
HIPAA Encrypted Deep-link
L3
Rationale
Reasoning Path
Hidden behind hover/dwell interaction to reduce visual noise. Reveals the computational logic and decision tree that led to this insight, maintaining transparency without overwhelming the interface
TOON-AI Semantic Engine
L4
Evidence
Source Attribution
Direct deep-link to source EHR record with HIPAA encryption. Enables immediate audit trail and source verification, critical for clinical decision support and regularity compliance.
JSON-AI Evidence Engine
JSON-AI (Evidence Engine)
TOON-AI (Semantic + Logic)
Core Flow Walkthrough
Interaction Map & Progressive Disclosure
Progressive disclosure: from ambient awareness to clinical decision
Two UI patterns: Continuity Strip (State 1-3) and Tieline Navigation (State 4)
State 1
Passive
The Glance
None
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
State 2
300ms Hover
The Lean-In (Dwell)
Hover
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
L3
Medication Discrepancy
Critical
Confidence: 94%
Metformin 1000mg BID found in CVS community record (filled 02/10), but missing from Epic chart. Patient reported taking medication during intake.
View Details
State 3
Click
The Audit (Action)
Click to expand
Patient: Sarah Chen
MRN: 847-2934 | Age: 67
Vitals
Notes
Labs
Medications
Imaging
Intelligence Stream
Medication Discrepancy Analysis

Evidence Deep-Dive
Source Comparison
Epic (Current)
No Metformin recorded
CVS Record
Metformin 1000mg BID
Filled: 02/10/2026
L4
Confidence: 94%
CVS_RX_2026-10_08:34:22
Prescription filled by Pharmacy ID: CVS-2847
Patient_Intake_2026-02-13_07:12:03
Verbal confirmation during admission
Epic_MedRec_Last_Updated_0225-11-03
Verbal confirmation during admission
Clinical Decision
Reconcile to Chart
Dismiss Alert
HIPAA Encrypted Deep-link
Continuity Strip: Progressive Disclosure
1
Passive Awareness
Ambient signals require zero cognitive load. Visual pulse communicates importance without interrupting workflows
2
contextual Insight
300ms dwell threshold reveals reasoning. Just-in-time information prevents alert fatigue while maintaining transparency
3
Verifiable Action
Full audit trail with clinical handshake. Every decision is traceable, reversible, and compliant with regulatory requirements
Shared Timeline
This isn’t a dashboard. It’s system memory
Why it exists
- Shift handoffs
- End-of-day review
- Cross-role reconciliation
What it shows
- Decisions and overrides
- AI insights with confidence
- Evidence trails across time
Systems Impact
Measuring Success
Validating continuity without increasing risk
What I’d Measure
Time to orientation
How quickly users understand what changed and what matters
Clarification loops
Back-and-forth caused by missing or unclear context
Scheduling failures
Downstream breakdowns caused by incomplete handoffs
AI insights acceptance vs override rates
A proxy for trust and signal quality
What I’d Test
- Confidence threshold tuning
- Role-based prioritization of insights
- Signal fatigue over time
Design Principle
AI earns trust by reducing work, not by demanding belief
Risks & Open Questions
Designing AI for real-world systems, not ideal conditions
Human Reality
- Trust must be earned
- Workflow disruption causes rejection
- Training and change fatigue are real
Integration Reality
- Varying EMR capabilities
- Limited control over host UI
- Long enterprise deployment cycles
Data Reality
- Incomplete records
- conflicting sources
- delayed or stale inputs
Design Responses & Mitigations
Core
Low Risk
Sidecar architeture
(low integration risk)
Alert
Info
Visual separation from system alerts
CTRL
Explicit human confirmation and override
Let’s Work Together
Interested in collaborating on complex UI/UX challenges involving data, AI, or enterprise systems?
I’d love to explore how thoughtful design can drive clarity and business impact.

Get In Touch

About Kelli
Product Designer | AI x Data Systems
Passionate about turning complex data and AI systems into clear, trustworthy, human-centered experiences
Based in: San Francisco, CA
© 2026 Kelli Nordfelt